
This medical malpractice case is high yield for every emergency physician as it covers a subtle but life-threatening diagnosis and highlights the importance of communication at multiple levels. It also provides an opportunity for us to better understand the nuances of EMTALA-related litigation.
Explore This Issue
ACEP Now: Vol 39 – No 12 – December 2020The Case
A 30-year-old man presented to the emergency department with a chief complaint of weakness and ankle pain. He was seen in an outpatient clinic and referred to the emergency department for evaluation. The patient had recently returned from a surfing trip to Asia. While on the trip, he reported being bitten by mosquitos multiple times but had not taken any malaria prophylaxis. He also had jumped out of a truck the day before and had twisted his left ankle.
The review of systems was positive for fever, vomiting, myalgias, and headaches.
He was otherwise healthy and up-to-date on his vaccinations.
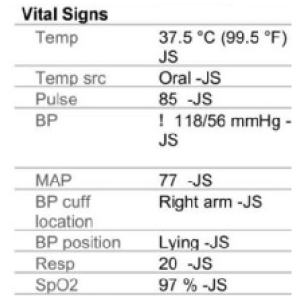
Figure 1
His triage vitals showed a temperature of 99.5ºF, heart rate of 85 bpm, blood pressure of 118/56, respirations of 20 per minute, and oxygen saturation of 97 percent on room air (see Figure 1).
A boilerplate normal examination was documented, including a musculoskeletal note describing “no edema and no tenderness.”
The physician noted a differential of “viral syndrome, otitis media, pharyngitis, pneumonia, gastroenteritis, urinary tract infection, and others.”
A complete blood count (CBC) was ordered and showed leukocytosis of 14.9, thrombocytopenia of 132. The differential showed 87 percent neutrophils and 5 percent lymphocytes. The comprehensive metabolic panel (CMP) was entirely unremarkable. The urinalysis showed a large amount of blood and occasional bacteria but no white blood cells, leukocyte esterase, or nitrites. An influenza swab was negative, and a malaria smear was also negative (see Figure 2).
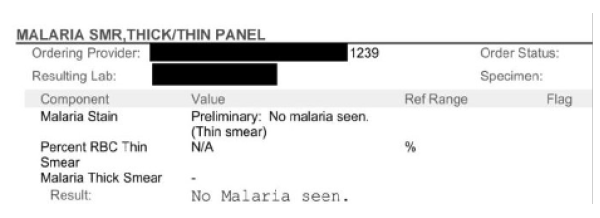
Figure 2
An ankle X-ray was ordered and showed “moderate soft tissue swelling” but no fracture or dislocation.
A repeat set of vitals was ordered, and everything was in the normal ranges.
Given the lack of emergency findings and normal vitals, the patient was discharged home. The doctor recommended he take Tylenol or ibuprofen, stay hydrated, and rest. Crutches were provided, and instructions were given to keep the left ankle elevated. A plan to follow up with urgent care the following week for reassessment was recommended.
Commentary
Everything about this case seems straightforward to this point. There is nothing that can be reasonably criticized. The workup is negative.
But this is a medical malpractice column. There has to be a twist.
Recall that the patient was seen in an outpatient clinic and referred to the emergency department. The ED physician was unaware of this. The patient did not volunteer this information, there were no triage notes mentioning it, and no one asked the patient about the preceding medical care.
Shortly before ED arrival, the outpatient clinic documented a blood pressure of 81/38 and a temperature of 100.2ºF.
Pages: 1 2 3 | Single Page




No Responses to “What Is—and Isn’t—Guaranteed Under EMTALA Can Be Complex”