
Does Zika infection cause fetal malformations? In Brazil, the incidence of microencephaly is not clearly known. However, during the current outbreak, observations suggest a possible 20-fold rise in this malformation over previous years. Some of the children with microencephaly tested positive for Zika; some did not. Although there is no absolute confirmation of a link between Zika and fetal malformations, the latest report by the U.S. Centers for Disease Control and Prevention (CDC) greatly strengthens the theory. However, the circumstantial evidence is concerning enough that multiple agencies have issued alerts to people living in or planning to travel to Zika outbreak areas. Additionally, increasing incidences of Guillain-Barre syndrome have been reported in the Zika outbreak areas. The CDC is also investigating this potential association. No link has yet been confirmed, but as with any viral syndrome later developing neurologic findings, this entity should be considered.
Explore This Issue
ACEP Now: Vol 35 – No 04 – April 2016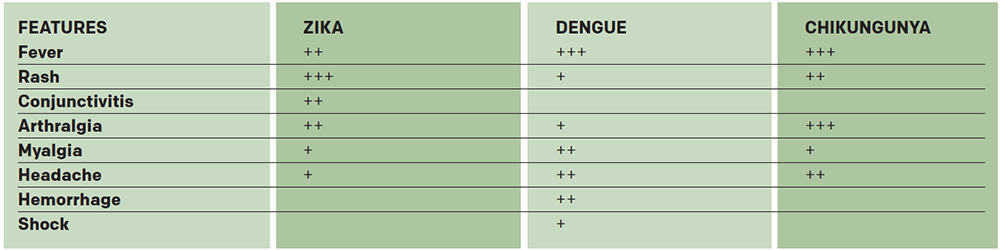
(click for larger image) Table 1. Differential Diagnosis Based on Clinical Presentation of Three Emerging Flaviviral Diseases
Source: CDC
Testing and Treatment
Treatment of Zika is entirely symptomatic. No vaccine exists for Zika. Vaccines for other flaviviruses (yellow fever, Japanese encephalitis, tickborne encephalitis, and dengue) are available but are of no benefit in Zika. Several companies are working on a Zika vaccine. Because the primary concern is in pregnancy, additional burden is placed on vaccine creators to ensure the safety and efficacy for the mother and fetus. It is probable that a vaccine is at least two years away, but it will likely be longer.
Testing is available for Zika through the CDC and should be performed based on the most current guidelines provided by that agency. Pregnant women who have a travel history to an outbreak area should be tested. All Zika testing is done through state or local departments of health and should be coordinated through those agencies. In settings where the clinician is considering testing outside of the above recommendation, consultation with the state or local epidemiologist on call is indicated. The assay is specific for Zika immunoglobulin M (IgM) antibodies. Such antibodies are detectable between four days and 12 weeks following infection. The results are available within one to two weeks. A positive test only means that the Zika IgM antibody has been detected. It says nothing about the clinical condition of the patient or fetus or the risk of a fetus developing a malformation. False-positive tests are possible after a recent infection with a related flavivirus or in people who have received yellow fever or Japanese encephalitis vaccines. This means that a positive Zika IgM test must be confirmed by other testing at the CDC. Any positive test is an indication for careful referral of pregnant patients to obstetrics/gynecology and patient counseling as outlined by the CDC.
Pages: 1 2 3 | Single Page




One Response to “Zika Virus Transmission, Testing, and Treatment Information You Need to Know”
May 8, 2016
David MorganExcellent update.