This is the second in a multi-part ACEP Now series focused on mental health emergencies. Last month’s article focused on ACEP’s efforts and resources to support EDs and patients with psychiatric emergencies. Future articles will highlight solutions and success stories. This month, we are discussing the medical management of patients with mild to moderate agitation.
Explore This Issue
ACEP Now: Vol 42 – No 07 – July 2023Emergency departments (EDs) focus on rapid initiation of medical treatment. Patients with sepsis get antibiotics. Patients with opiate overdose get naloxone. Patients in DKA get insulin. And yet, when many patients arrive with a mental health crisis, they get nothing—until they escalate, at which point they often get too much and remain over-sedated for hours. Just as for patients experiencing other emergencies, ED physicians should rapidly initiate appropriate medical treatment for patients experiencing mental health crises, before they decompensate.
Calming Measures
Sometimes ED physicians are reluctant to initiate calming treatment in lower acuity patients, preferring to wait until more aggressive sedation is absolutely necessary. They might have been instructed that early calming measures lead to an inaccurate evaluation of the patient by a mental health professional or worry about over-sedating the patient. However, rapid initiation of treatment is actually patient-centered care that can both lead to better outcomes and limit ED boarding. Mental health evaluation teams can rely on documentation and interviews to understand a patient’s initial agitation level. It is also equally important for mental health evaluators to understand how patients respond to calming medication, as that can help guide inpatient versus outpatient treatment decisions.
This article focuses on calming medication in patients with mild to moderate agitation. The article also will not address severe agitation, which is already well covered elsewhere and is the topic of an ACEP clinical policy currently in development.1–3
When to Consider Calming Treatments
Calming treatment should be considered immediately upon arrival for patients who are experiencing agitation or anxiety, even if the symptoms are not severe.4 The first step is to establish a therapeutic alliance and engage in verbal de-escalation.5 ED physicians should use a calm, non-confrontational tone, respect the patient’s personal space, set polite but firm boundaries for behavior, and offer choices where appropriate. Sometimes investing an extra two to five minutes—certainly a significant time commitment on a busy shift—to establish trust can limit the need to spend even more time later in the shift managing escalating behavior (or permit a much earlier disposition).
Once trust is established and patients are willing to accept calming medication, emergency physicians should consider these guiding principles.
First, oral administration is preferred, as this route can often be as effective as intramuscular administration.6,7 Oral medications are typically cheaper, easier for the patient, reduce the risk of needlesticks, and limit plastic waste.
Second, to avoid increased side effects, the dosing should usually start lower, especially for elderly patients. Treatment should typically begin with just one agent, rather than multiple different medications.8
Third, patients may express a preference for a specific medication or dose based on prior experience. As long as this request is not for a narcotic or other medication with potential secondary gain, it should be respected if feasible.
Fourth, ED treatment should be approached as the first step in a long-term treatment plan, and not as an isolated decision confined to just the ED stay. This means that for patients who have outpatient prescriptions, preference should be given to reinitiating those medications in the ED if feasible, instead of starting a different regimen.
Finally, other interventions focused on comfort should also be considered. These might include medications such as ibuprofen, acetaminophen, or nicotine patches. Meals should be offered, especially if the patient will have a prolonged stay. Environmental stimuli, such as noise and light, should be minimized as possible.
Exceptions

Click to enlarge.
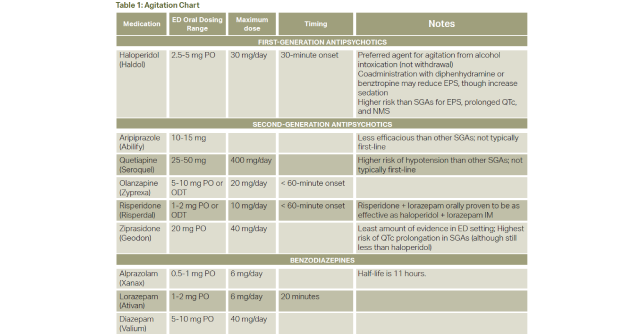
Certainly, each of these guiding principles has clear exceptions, and treatment decisions are at the discretion of the ED physician. For patients with mild to moderate agitation, treatment often begins with second generation antipsychotics (SGAs).9–11 Surprisingly to many ED physicians, these meds are preferred over first-generation antipsychotics (FGAs) such as haloperidol given a lower risk of extrapyramidal symptoms and QTc prolongation. Common injectable SGAs with evidence in the ED setting include olanzapine or ziprasidone, or if oral, risperidone. Of these, olanzapine and ziprasidone are most frequently used in the ED setting for mild to moderate agitation. Aripiprazole for acute agitation is approximately as efficacious as lorazepam, and quetiapine has a higher risk of orthostatic hypotension. Table 1 reviews common dosing regimens and notable side effects.
Benzodiazepines are also frequently used, though ideally not concomitantly with SGAs in patients who have alcohol intoxication.12 Benzodiazepines are ideal for patients whose agitation is due to stimulant use or alcohol withdrawal. They may also be preferred in patients with an unknown etiology for agitation. However, when agitation is due to an underlying psychiatric disorder, SGAs are preferred.
Finally, once patients with mild to moderate agitation are stabilized and ready for discharge, the ED physician should consider re-starting outpatient medications. While the initiation of a new outpatient antipsychotic regimen is beyond the scope for most ED physicians, it is certainly reasonable for ED physicians to refill or restart an existing medication regimen.
 Dr. Miller is Chief Medical Officer of Vituity. Dr. Miller leads an EMPC sub-committee focused on mental health issues in the ED.
Dr. Miller is Chief Medical Officer of Vituity. Dr. Miller leads an EMPC sub-committee focused on mental health issues in the ED.
 Dr. Enguidanos is Chair of ACEP’s Emergency Medicine Practice Committee (EMPC). He is Founder/CEO of Community Based Coordination Solutions.
Dr. Enguidanos is Chair of ACEP’s Emergency Medicine Practice Committee (EMPC). He is Founder/CEO of Community Based Coordination Solutions.
 Dr. Wilson is board-certified in emergency medicine and is an associate professor (tenured) in the Departments of Emergency Medicine and Psychiatry at the University of Arkansas for Medical Sciences.
Dr. Wilson is board-certified in emergency medicine and is an associate professor (tenured) in the Departments of Emergency Medicine and Psychiatry at the University of Arkansas for Medical Sciences.
References
- American College of Emergency Physicians Clinical Policies Subcommittee on the Adult Psychiatric P, Nazarian DJ, Broder JS, et al. Clinical Policy: Critical Issues in the Diagnosis and Management of the Adult Psychiatric Patient in the Emergency Department. Ann Emerg Med. Apr 2017;69(4):480-498.
- Wilson MP, Pepper D, Currier GW, Holloman GH, Jr., Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. Feb 2012;13(1):26-34.
- Schneider A, Mullinax S, Hall N, Acheson A, Oliveto AH, Wilson MP. Intramuscular medication for treatment of agitation in the emergency department: A systematic review of controlled trials. Am J Emerg Med. Aug 2021;46:193-199.
- Zun L, Wilson MP, Nordstrom K. Treatment Goal for Agitation: Sedation or Calming. Ann Emerg Med. Nov 2017;70(5):751-752.
- Richmond JS, Berlin JS, Fishkind AB, Holloman GH Jr, Zeller SL, Wilson MP, Rifai MA, Ng AT. Verbal De-escalation of the Agitated Patient: Consensus Statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup. West J Emerg Med. 2012 Feb;13(1):17-25.
- Mullinax S, Shokraneh F, Wilson MP, Adams CE. Oral Medication for Agitation of Psychiatric Origin: A Scoping Review of Randomized Controlled Trials. J Emerg Med. Oct 2017;53(4):524-529.
- Currier GW, Chou JC, Feifel D, et al. Acute treatment of psychotic agitation: a randomized comparison of oral treatment with risperidone and lorazepam versus intramuscular treatment with haloperidol and lorazepam. J Clin Psychiatry. Mar 2004;65(3):386-94.
- Zaman H, Sampson SJ, Beck AL, et al. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Database Syst Rev. Dec 8 2017;12(12):CD003079.
- American College of Emergency Physicians Clinical Policies Subcommittee on the Adult Psychiatric P, Nazarian DJ, Broder JS, et al. Clinical Policy: Critical Issues in the Diagnosis and Management of the Adult Psychiatric Patient in the Emergency Department. Ann Emerg Med. Apr 2017;69(4):480-498.
- Roppolo LP, Morris DW, Khan F, Downs R, Metzger J, Carder T, Wong AH, Wilson MP. Improving the management of acutely agitated patients in the emergency department through implementation of Project BETA (Best Practices in the Evaluation and Treatment of Agitation). J Am Coll Emerg Physicians Open. 2020 Jul 3;1(5):898-907.
- Wilson MP, Pepper D, Currier GW, Holloman GH Jr, Feifel D. The psychopharmacology of agitation: consensus statement of the american association for emergency psychiatry project Beta psychopharmacology workgroup. West J Emerg Med. 2012 Feb;13(1):26-34.
- Wilson MP, Chen N, Vilke GM, Castillo EM, MacDonald KS, Minassian A. Olanzapine in ED patients: differential effects on oxygenation in patients with alcohol intoxication. Am J Emerg Med. Sep 2012;30(7):1196-201.
Pages: 1 2 3 4 | Multi-Page



One Response to “Agitation Treatment in the Emergency Department”
July 12, 2023
John SmithI appreciate the article’s emphasis on the importance of early intervention in the treatment of agitation. Agitation can quickly escalate, so it is important to intervene early to prevent a patient from becoming more aggressive or violent.