A 59-year-old male with a past medical history of a repaired ventricular septal defect (VSD), dextrocardia, hypertension, hyperlipidemia, and current smoker presented to the emergency department (ED). This patient had known coronary artery disease (CAD), and previously required drug eluting stents to the obtuse marginal and diagonal arteries. The patient expressed epigastric pain, nausea, and fatigue followed by non-exertional, constant right-sided chest pain with radiation to his right arm.
Explore This Issue
ACEP Now: Vol 43 – No 04 – April 2024The patient initially presented to an outside ED and was subsequently transferred to our facility for continuity of care. Patient had stable vital signs with an oral temperature of 36.4 degrees Celsius, heart rate of 91, blood pressure of 118 over 76, respiratory rate of 23, and pulse ox of 96 percent on room air. He was asymptomatic upon presentation.
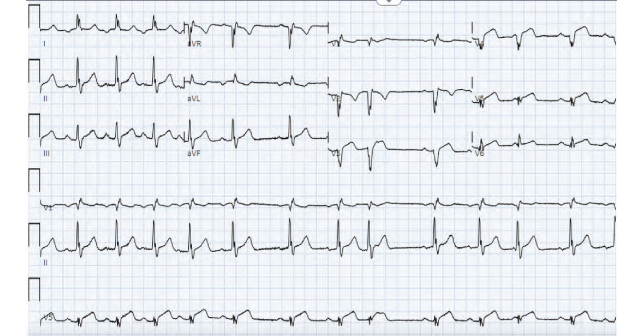
A traditional, left-sided EKG was initially obtained, which demonstrated inverted P waves in lead I, deep Q waves in lead V1, negative QRS complex in V1, and RBBB. It was immediately discerned that the patient had dextrocardia from previous records, and an EKG for dextrocardia was obtained.
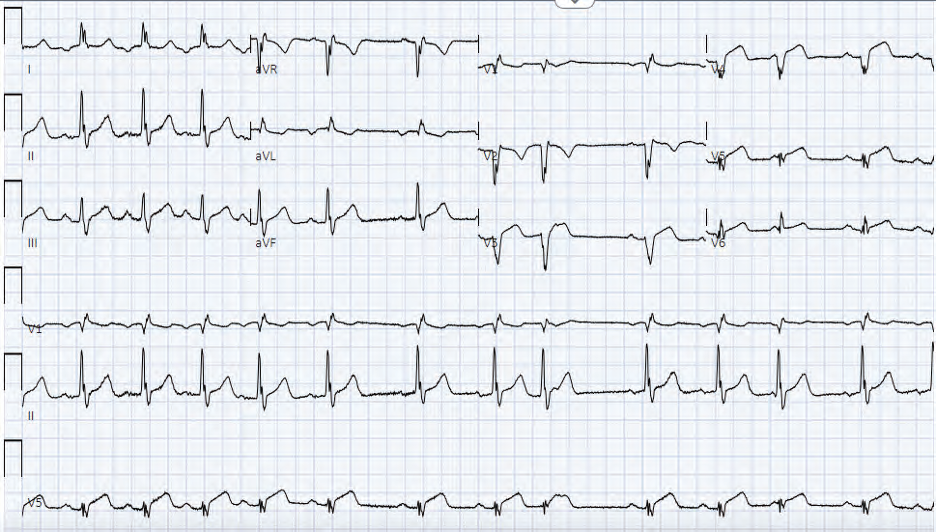
Figure 1: EKG for Dextrocardia showing STEMI. (Click to enlarge.)
The second EKG was concerning for STEMI in the precordial leads (see figure 1). The patient’s first and second troponins from the outside hospital were less than 0.01 ng/mL. The third troponin at our facility resulted as greater than 50.00 ng/mL. The patient was started on IV heparin and immediately taken for cardiac catheterization.
In the cath lab, the patient was found to have evidence of a proximal thrombus and significant stenosis of the LAD (see figure 2). He underwent successful revascularization and stenting of the proximal to mid LAD.
Discussion

Figure 2: Cardiac cath. (Click to enlarge.)
Dextrocardia is a rare congenital anomaly where the heart is intrinsically positioned in the right hemithorax with the apex pointing towards the right caudal position.1 It has a prevalence of 0.01 percent.1 Dextrocardia can be associated with an overall situs inversus, where all internal organs are in the reversed position or be limited to situs ambiguous, where only some organs are in the reversed.1
Despite the rarity of dextrocardia, coronary artery disease can occur with a similar frequency to that of the general population.3 Coronary artery disease in a patient with Dextrocardia can present with particular findings on a traditional left-sided EKG that raise suspicion for this anomaly. However, there may be diagnostic dilemmas if these findings are not immediately recognized. This delay in recognition can result in the inadvertent underdiagnosis of STEMIs. Thus, it is important to recognize dextrocardia and adjust our diagnostic tools appropriately.
Pages: 1 2 3 | Single Page



No Responses to “Case Report: A Rare Congenital Heart Anomaly”