
A healthy 20-year-old male presented with one day of a progressively worsening sore throat with difficulty swallowing, increased secretions, and increased work of breathing. He had no history of allergies, anaphylaxis, or recent dental procedures or infection. He endorsed daily inhalational marijuana usage.
Explore This Issue
ACEP Now: Vol 43 – No 11 – November 2024Description of Diagnosis, Management

Figure 1. Large uvular swelling on pharyngeal exam. (Click to enlarge.)
On examination, he had a significantly enlarged uvula with erythema and edema. His voice sounded muffled. He had mild ecchymosis along the medial soft palate with superficial mucosal irritation. He had no tonsillar edema or exudate. The tongue and lips were normal in size without any swelling. No brawny edema to the submental region. He was tachypneic with increased salivation, but he was able to manage his secretions. The remainder of the exam was unremarkable.
His initial workup consisted of close airway observation with end-tidal capnometry, rapid strep test, throat culture, respiratory pathogens PCR, and a neck X-ray. A bedside nasopharyngoscopy was conducted; it showed crisp tonsillar structures and no laryngeal edema. A diagnosis of uvulitis was given.
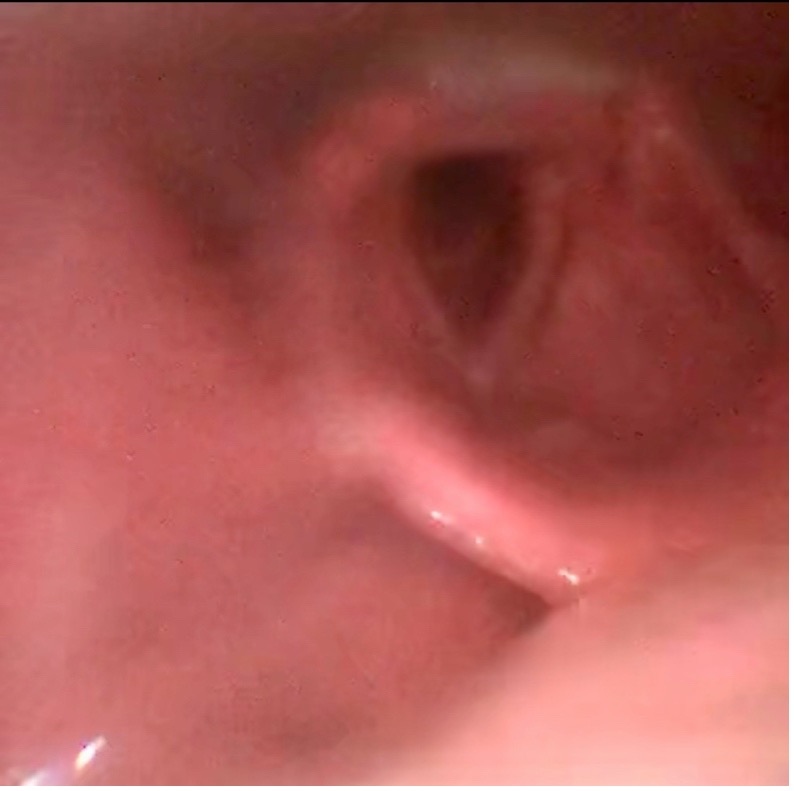
Figure 2. Still image captured from nasopharyngoscopy showing no laryngeal edema. (Click to enlarge.)
After this, close airway monitoring was continued and, given the degree of uvular edema and increased secretions, we empirically treated the patient with intravenous (IV) antibiotics (ampicillin-sulbactam), corticosteroids, antihistamines.
The laboratory testing and neck X-ray were unremarkable for any acute infectious etiology. The patient was admitted to the hospital for airway observation. The uvular edema resolved in 24 hours and the patient was discharged on a course of oral corticosteroids and oral antibiotics.
Uvulitis is inflammation of the uvula that is often caused by the spread of an underlying oropharyngeal infection, such as pharyngitis or epiglottitis. Populations such as young children, unvaccinated or undervaccinated patients, and patients with poor dentition are at an increased risk for developing uvulitis. However, isolated uvulitis is highly unusual and has a possible association with inhalational drug use.1

Figure 3. Still image captured from nasopharyngoscopy showing crisp vocal cords and tonsillar fornixes. (Click to enlarge.)
A review of the literature shows cases of isolated uvulitis occurring in the setting of habitual inhalational drug use such as marijuana, fentanyl, or methamphetamine.2 These cases depict isolated enlargement, erythema, and edema of the uvula. In some cases, the clinical presentation worsened, resulting in acute airway obstruction requiring treatment with empiric antibiotics, racemic epinephrine, intravenous (IV) corticosteroids, and antihistamines with close airway observation.
Patients with isolated uvulitis often present with an erythematous, edematous, and enlarged uvula with crisp surrounding structures; it can be accompanied by fever, odynophagia, dysphagia, difficulty managing secretions, and possibly respiratory distress.3 Treatment of uvulitis typically consists of IV corticosteroids, racemic epinephrine, antihistamines, empiric antibiotics, and close airway monitoring.
This case exemplifies that uvulitis, despite its rarity, should be considered in the differential diagnosis for patients with respiratory distress or airway swelling, especially as we see a rise in the use of inhalational marijuana and other recreational drugs. Workup and treatment of isolated uvulitis should include consideration of infectious etiologies as well as inhalational etiologies. The use of nasopharyngoscopy, performed by a skilled clinician, is extremely helpful to evaluate the extend of the edema and the presence of tonsillar and laryngeal involvement.4
As with any airway emergency, advanced airway supplies, close airway monitoring, and temporizing agents should be used to empirically treat the patient and secure the airway. In this case, the patient’s symptoms improved with empiric antibiotics, corticosteroids, and antihistamines. However, consideration may be given to racemic epinephrine, as demonstrated in other case reports. We also advocate for an admission for close airway observation until the edema has resolved, cessation of all inhalational drug use, and close follow-up with otolaryngology.
Teaching Points
- Ask about inhalational drug use if a patient presents with isolated uvulitis.
- Broad treatment with steroids, IV antibiotics, antihistamines, and possibly racemic epinephrine should be considered until the etiology is determined.
- Use of nasopharyngoscopy is useful for excluding angioedema of vocal cords, epiglottis and larynx.
 Dr. Keswani is an emergency medicine resident at the Department of Emergency Medicine at University of Virginia Health System.
Dr. Keswani is an emergency medicine resident at the Department of Emergency Medicine at University of Virginia Health System.
 Dr. Mutter is an associate professor at the Department of Emergency Medicine at University of Virginia School of Medicine.
Dr. Mutter is an associate professor at the Department of Emergency Medicine at University of Virginia School of Medicine.
 Dr. Smith is an assistant professor at the Department of Emergency Medicine at University of Virginia School of Medicine.
Dr. Smith is an assistant professor at the Department of Emergency Medicine at University of Virginia School of Medicine.
References
- Rawal SY, Tatakis DN, Tipton DA. Periodontal and oral manifestations of marijuana use. J Tenn Dent Assoc. 2012;92(2):26-31.
- Boyce SH, Quigley MA. Uvulitis and partial upper airway obstruction following cannabis inhalation. Emerg Med (Fremantle).2002;14(1):106-108.
- Shiber JR, Fontane E. Quincke’s Disease: isolated uvulitis. West J Emerg Med.2014;15(6):663.
- Fappiano C, Inman BL, Bridwell RE. Isolated uvulitis in a patient after smoking fentanyl. Cureus. 2023;15(4):e38109.
Pages: 1 2 | Multi-Page



No Responses to “Case Report: Uvular Edema in a Marijuana Smoker”