
Increasing use of CT is concerning due to radiation exposure, and patients with recurrent renal colic are at particularly high risk of repeat CTs, with a median dose of 7.9 mSv each (20 mSv is the maximum allowable for radiation workers annually, and 100 mSv is associated with carcinogenic effects).
Explore This Issue
ACEP Now: Vol 33 – No 01 – January 2014The cost of these CTs adds up to real dollars. In 2012, Medicare reimbursement for non-contrast CT of the abdomen was $306, while hospital charges ranged from $35 to $2,724. In 2009, an estimated 497,000 CTs were performed for the evaluation of renal colic, totaling $152 million in medical costs (a conservative estimate based on Medicare payments).3
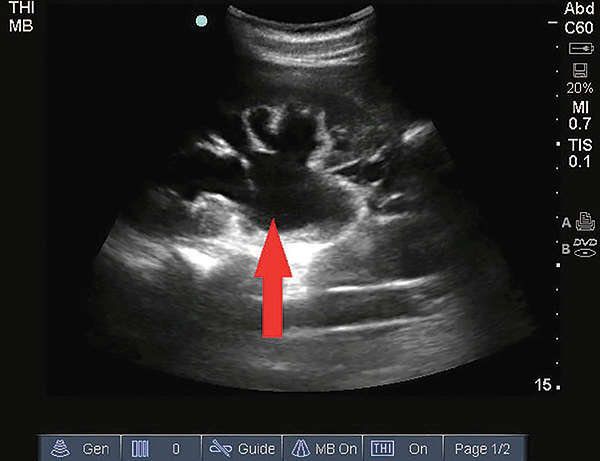
Hydronephrosis appears on ultrasound as a dilated hypoechoic (black) region in the collecting system of the kidney.
How can we safely evaluate patients with recurrent renal colic in a more cost-effective way than with repeat CTs?
Urinalysis and bedside renal ultrasound are an effective strategy to confirm recurrent renal colic. Microscopic hematuria is found in 84 percent of patients with kidney stones; however, due to its presence in other diseases, the specificity is 48 percent. Adding ultrasound enhances the yield of urinalysis alone.
Bedside ultrasound by an emergency physician is rapid, safe, and less expensive than CT. Ultrasound is 87 percent sensitive and 82 percent specific for the identification of hydronephrosis, which is present in 69 percent of patients with acute ureteral colic.4 While ultrasound is less sensitive for the detection of small stones, you don’t need to see the stone to make the diagnosis of renal colic. If you choose to perform ultrasound instead of CT, you aren’t alone—the American College of Radiology appropriateness criteria rates ultrasound as equivalent to CT of the abdomen for the evaluation of recurrent stones. If your group and emergency department are billing for ultrasounds, the cost of a renal ultrasound based on Medicare rates is $99, less than a third of the cost of CT.
With basic training, hydronephrosis is easy to identify using ultrasound. In one study, second-year emergency-medicine residents were able to identify hydronephrosis with 96 percent accuracy compared to registered sonographers after 45 minutes of renal ultrasound training (within a larger curriculum).5 Not all renal colic patients need IV fluids, but hydronephrosis is easier to detect after a 500 cc bolus. A prospective study of urinalysis and ultrasound in 227 patients resulted in discharge of half of patients found to have hydronephrosis and microscopic hematuria.6 Among those discharged, 81 percent ultimately had kidney stones, and none had adverse outcomes within three months.
The Bottom Line
The emergency physician’s role in the management of acute renal colic is symptom relief, evaluation for complications such as infection, and consideration of alternate diagnoses. The vast majority of stones pass spontaneously, and CT imaging in the emergency department rarely alters immediate management. One randomized study found that patients with suspected renal colic who undergo delayed outpatient imaging have equivalent outcomes to those who undergo emergency department imaging at four-week follow-up.7
Pages: 1 2 3 | Single Page





No Responses to “A Cost-effective Way to Evaluate Patients with Recurrent Renal Colic”