
Urinalysis and bedside renal ultrasound are effective, safe, and less expensive than repeat CT scans
“Doctor, EMS just brought a man who is really uncomfortable into bay 4. He looks like he has a kidney stone, and he’s had one before. Can I give him some morphine?”
Explore This Issue
ACEP Now: Vol 33 – No 01 – January 2014“Sure, put him in for a CT, and I’ll see him in a few minutes.”
Every day, emergency departments across the United States care for similar patients. Kidney stones affect one in 11 adults in the United States, and their prevalence has increased 40 percent in the past decade. Renal colic accounts for more than 700,000 emergency-department visits annually, and in 2009, 71 percent of these patients underwent CT examination. Depending on how it’s measured, the use of CT for renal colic has increased between three- and tenfold in the last two decades.1,2
Among patients presenting with recurrent acute renal colic, should non-contrast CT of the abdomen be the standard diagnostic approach?
CT of the abdomen is the preferred diagnostic test to identify kidney stones due to its accuracy, speed, and widespread availability. Sensitivity ranges from 94 percent to 100 percent, while specificity ranges from 92 percent to 100 percent. CT is the test of choice for patients presenting with first-time renal colic or potentially complicated renal colic (eg, fever, a single kidney, or immunosuppression). Additionally, in patients in whom you suspect a serious alternate cause of their flank pain (eg, dissecting abdominal aortic aneurysm), CT should be performed. However, while CT is useful to detect extra-renal pathology, the rapid increase in CT use has not resulted in an increased incidence of alternate pathologies.
Increasing use of CT is concerning due to radiation exposure, and patients with recurrent renal colic are at particularly high risk of repeat CTs, with a median dose of 7.9 mSv each (20 mSv is the maximum allowable for radiation workers annually, and 100 mSv is associated with carcinogenic effects).
The cost of these CTs adds up to real dollars. In 2012, Medicare reimbursement for non-contrast CT of the abdomen was $306, while hospital charges ranged from $35 to $2,724. In 2009, an estimated 497,000 CTs were performed for the evaluation of renal colic, totaling $152 million in medical costs (a conservative estimate based on Medicare payments).3
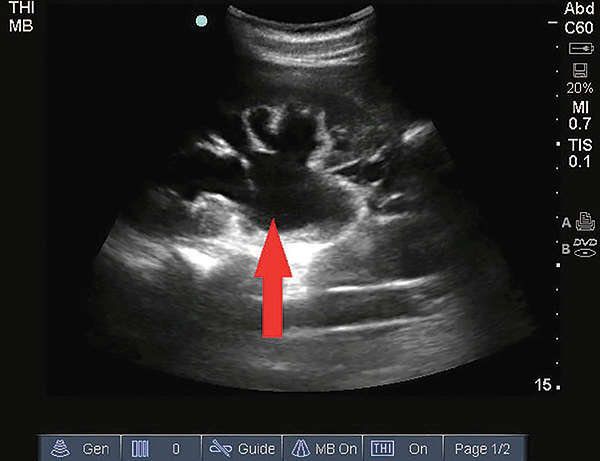
Hydronephrosis appears on ultrasound as a dilated hypoechoic (black) region in the collecting system of the kidney.
How can we safely evaluate patients with recurrent renal colic in a more cost-effective way than with repeat CTs?
Urinalysis and bedside renal ultrasound are an effective strategy to confirm recurrent renal colic. Microscopic hematuria is found in 84 percent of patients with kidney stones; however, due to its presence in other diseases, the specificity is 48 percent. Adding ultrasound enhances the yield of urinalysis alone.
Bedside ultrasound by an emergency physician is rapid, safe, and less expensive than CT. Ultrasound is 87 percent sensitive and 82 percent specific for the identification of hydronephrosis, which is present in 69 percent of patients with acute ureteral colic.4 While ultrasound is less sensitive for the detection of small stones, you don’t need to see the stone to make the diagnosis of renal colic. If you choose to perform ultrasound instead of CT, you aren’t alone—the American College of Radiology appropriateness criteria rates ultrasound as equivalent to CT of the abdomen for the evaluation of recurrent stones. If your group and emergency department are billing for ultrasounds, the cost of a renal ultrasound based on Medicare rates is $99, less than a third of the cost of CT.
With basic training, hydronephrosis is easy to identify using ultrasound. In one study, second-year emergency-medicine residents were able to identify hydronephrosis with 96 percent accuracy compared to registered sonographers after 45 minutes of renal ultrasound training (within a larger curriculum).5 Not all renal colic patients need IV fluids, but hydronephrosis is easier to detect after a 500 cc bolus. A prospective study of urinalysis and ultrasound in 227 patients resulted in discharge of half of patients found to have hydronephrosis and microscopic hematuria.6 Among those discharged, 81 percent ultimately had kidney stones, and none had adverse outcomes within three months.
The Bottom Line
The emergency physician’s role in the management of acute renal colic is symptom relief, evaluation for complications such as infection, and consideration of alternate diagnoses. The vast majority of stones pass spontaneously, and CT imaging in the emergency department rarely alters immediate management. One randomized study found that patients with suspected renal colic who undergo delayed outpatient imaging have equivalent outcomes to those who undergo emergency department imaging at four-week follow-up.7
So the next time you see a patient writhing in pain, saying, “Doc, it’s like my last kidney stone,” think twice before ordering the CT. Provide pain relief, get a urinalysis, and if you have an ultrasound and know how to identify hydronephrosis, throw on the probe. Hematuria or hydronephrosis on the side of the patient’s pain can help confirm your strong clinical suspicion of kidney stone. If your patient has both, it’s even more likely. If you have a real suspicion of another serious problem or can’t make the patient feel well enough to go home, order a CT. Practicing cost-effective care for patients with recurrent renal colic will reduce your patients’ exposure to radiation and can shorten their length of stay, both of which will improve their satisfaction.
References
- Fwu CW, Eggers PW, Kimmel PL, et al. Emergency department visits, use of imaging, and drugs for urolithiasis have increased in the United States. Kidney Int. 2013;83:479-486.
- Westphalen A, Hsia RY, Maselli JH, et al. Radiological imaging of patients with suspected urinary tract stones: national trends, diagnoses, and predictors. Acad Emerg Med. 2011;18:699-707.
- 2013 OPPS NPRM Cost Statistics Files for CPT 74176/ APC 0331. Centers for Medicare and Medicare Services. Accessed on December 5, 2013. Available at: http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/HospitalOutpatientPPS/Hospital-Outpatient-Regulations-and-Notices-Items/CMS-1589-P.html.
- Dalziel JP, Noble VE. Bedside ultrasound and the assessment of renal colic: a review. Emerg Med J. 2013;30:3-8.
- Mandavia DP, Aragona J, Chan L. Ultrasound training for emergency physicians: a prospective study. Acad Emerg Med 2000;7:1008e14.
- Kartal M, Eray O, Erdogru T, Yilmaz S. Prospective validation of a current algorithm including bedside US performed by emergency physicians for patients with acute flank pain suspected for renal colic. Emerg Med J. 2006;23:341-344.
- Lindqvist K, Hellström M, Holmberg G, et al. Immediate versus deferred radiological investigation after acute renal colic: a prospective randomized study. Scand J Urol Nephrol. 2006;40:119-124.
 Dr. Lin is an attending emergency physician and a fellow in the Division of Health Policy Research and Translation in the Department of Emergency Medicine, Brigham and Women’s Hospital in Boston. She also serves as an instructor at Harvard Medical School.
Dr. Lin is an attending emergency physician and a fellow in the Division of Health Policy Research and Translation in the Department of Emergency Medicine, Brigham and Women’s Hospital in Boston. She also serves as an instructor at Harvard Medical School.
 Dr. Schuur is Vice Chair of Quality and Safety and Chief of the Division of Health Policy Research and Translation in the Department of Emergency Medicine, Brigham & Women’s Hospital in Boston. He also serves as assistant professor at Harvard Medical School.
Dr. Schuur is Vice Chair of Quality and Safety and Chief of the Division of Health Policy Research and Translation in the Department of Emergency Medicine, Brigham & Women’s Hospital in Boston. He also serves as assistant professor at Harvard Medical School.
Pages: 1 2 3 | Multi-Page





No Responses to “A Cost-effective Way to Evaluate Patients with Recurrent Renal Colic”