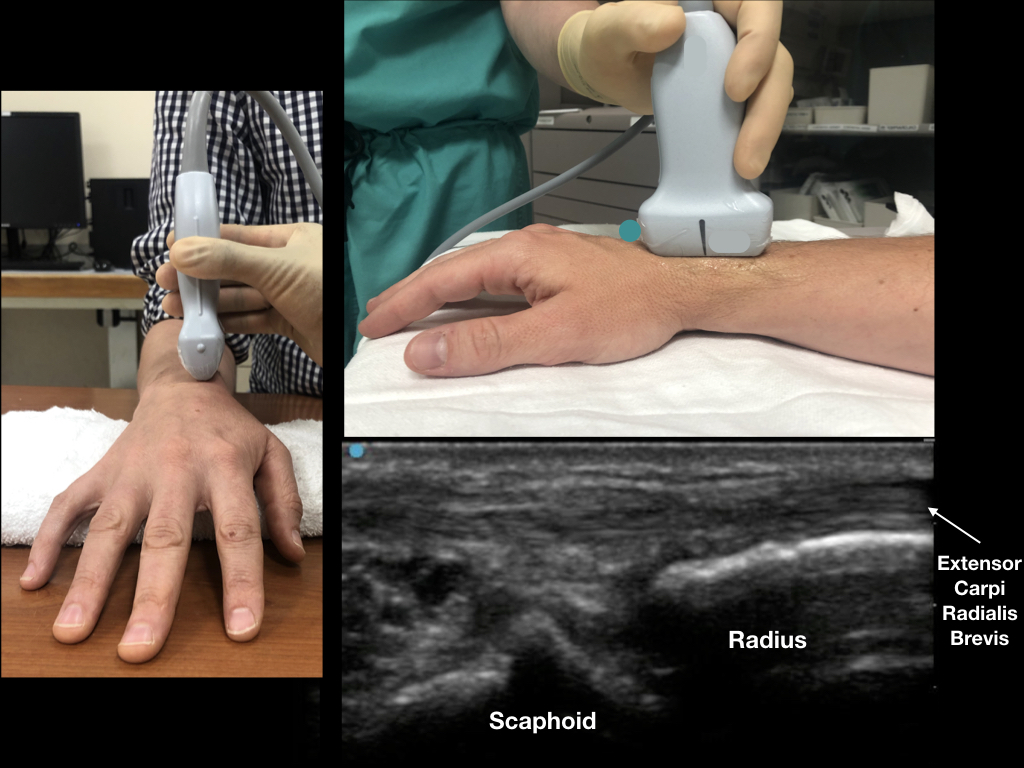
Figure 2: Rotate the ultrasound transducer in a longitudinal plane (compared to the radius) with the probe marker pointing distal. In a patient with no effusion, the distal radius and scaphoid bone with minimal anechoic fluid should be noted. Credit: Arun Naagdev
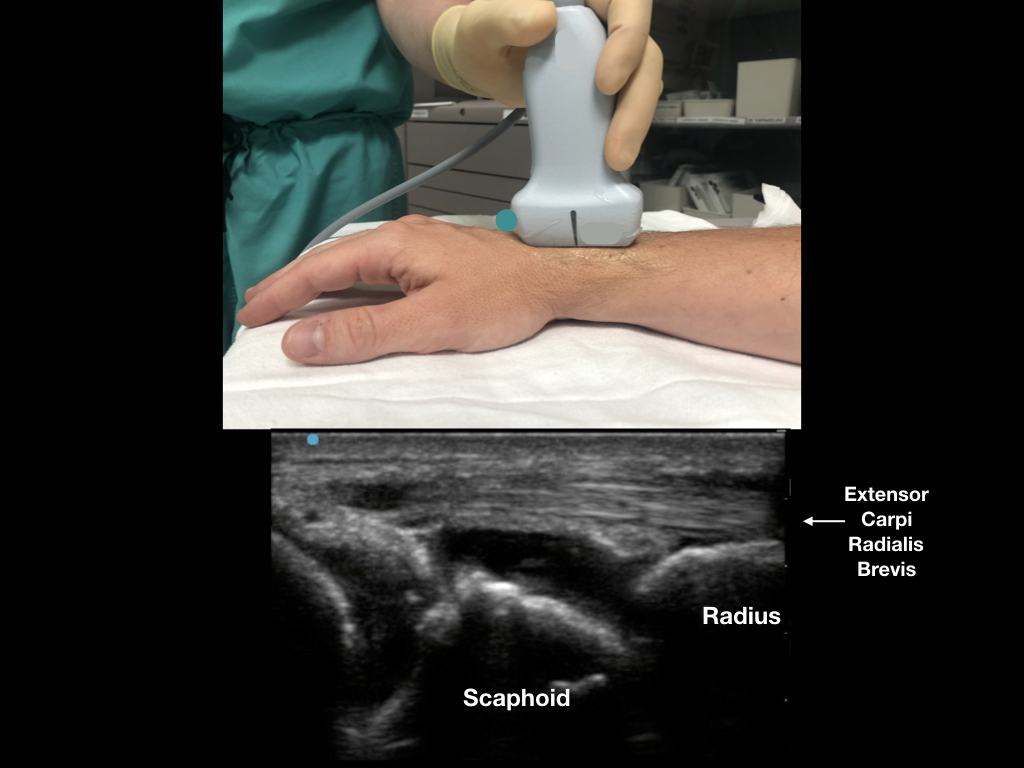
Figure 3: In a patient with a radiocarpal effusion, note the anechoic (black) fluid just anterior to the scaphoid. The extensor carpi radials brevis acts as a good ultrasound landmark. Credit: Arun Nagdev
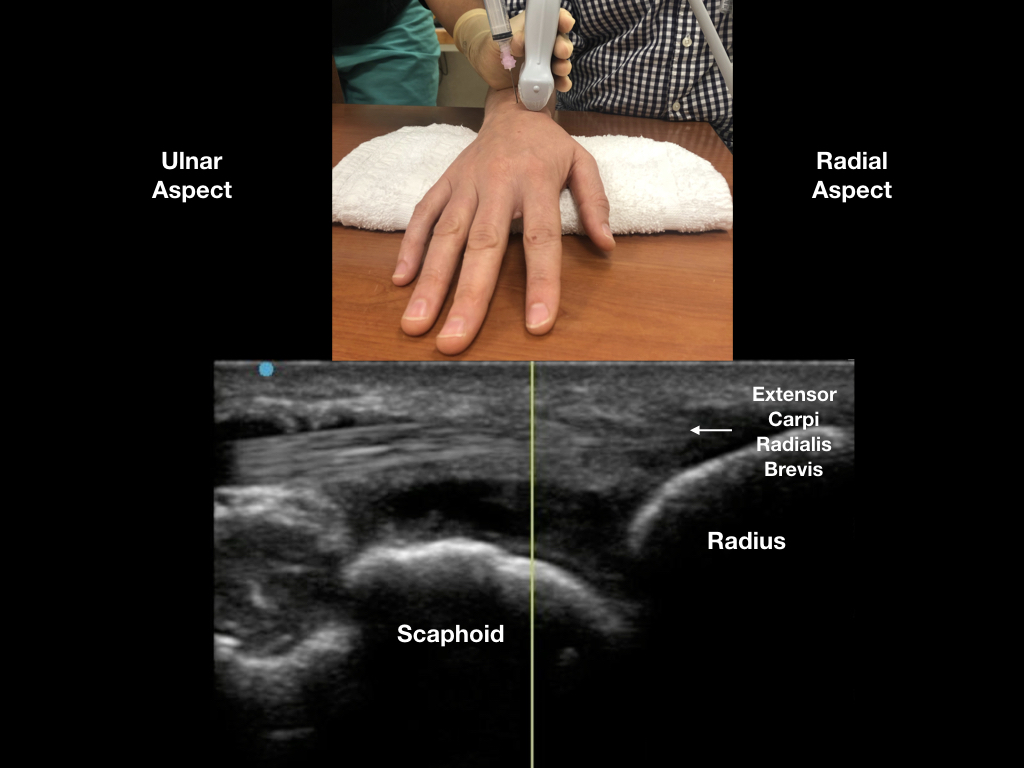
Figure 4: With the ultrasound probe covering the extensor carpi radials brevis, enter the swollen joint capsule with an out-of-plane technique. We recommend a steep needle angle of entry between Lister’s tubercle and the extensor carpi radials brevis. The procedure should be performed with sterile precautions (like any other joint aspiration). Credit: Arun Nagdev
Conclusion
The simplified technique described here gives clinicians inexperienced with wrist aspirations a reliable method to easily detect the presence of a joint effusion and, as needed, to enter the joint capsule with reduced risk of injury to tendons and vasculature. In our experience, this technique has been invaluable in the evaluation of patients with a painful and swollen distal forearm or wrist in our emergency department. In most cases, the clinician uses their physical exam in conjunction with ultrasound of the radiocarpal joint to determine the need for aspiration. In cases with a clear radiocarpal joint effusion, our novel, easy technique ensures successful joint fluid aspiration.
Pages: 1 2 3 | Single Page



No Responses to “Easy Ultrasound Technique to Evaluate and Aspirate an Atraumatic Painful Wrist”