For this month’s “Resident Voice” column, I explore how emergency medicine residents are innovating the field of medicine in creative and diverse ways. I requested residents to submit descriptions of their innovations, and was enthused at the breadth of initiatives being undertaken by emergency medicine residents across the country. I hope these three different initiatives which encompass research, community outreach, and technologic innovations will inspire you to pursue your own innovations.
Explore This Issue
ACEP Now: Vol 41 – No 03 – March 2022Starting a Nonprofit Organization

Dr. Coker
Sandra Coker, MD, PGY2, University of Chicago
My journey into medicine and to the founding of Black Girl White Coat surprisingly share a few things in common. I was the first in my family to pursue a career as an emergency physician, and I was also the first person I knew who had the audacity to start a nonprofit in the middle of it all. To be honest, I had no idea what to do, how to do it, or where to start with either endeavor. If we are being even more honest, I doubt I would have made it through undergraduate, medical school, and the nonprofit startup process if not for Google.
Despite my lack of experience and outside guidance, I always understood the incredible lack of people who looked like me doing the same jobs of which I dreamt.
My sole intention in founding Black Girl White Coat prior to beginning medical school in 2016 was to help provide resources and tools to Black students who either did not have the privilege of physician parents, resources to make their dreams come true, or the knowledge base to even get started. Studying human patterns shows us that we are most likely to become what we see and are surrounded by.1,2 Likewise, we have an easier time believing we can achieve something when we see other people who look like us achieve similar goals. This is a challenge for African American/Black and Latinx youth who grow up in communities where access to higher education comes at a much higher cost, mentorship is scarce, and exposure is limited.
In just five years, Black Girl White Coat has grown into a 501(c)3 organization that has helped over 600 Black and Latinx students through our mentorship program, awarded over $10,000 worth of scholarship to future health care professionals, and supplied numerous textbooks and other academic resources to those in need. Black and Latinx men and women are desperately needed to provide culturally competent quality care for a medical population that continues to grow in number and diversity. Support and representation have not previously been there; Black Girl White Coat exists to bridge that gap.
Black Girl White Coat is also exactly what I needed when I was younger. I hope everyone who encounters our organization soars to heights higher than I will ever reach. The potential has always been there; now we are tearing down barriers. However, we have more gaps to fill, especially when we look further down the line. More pipeline programs are needed in traditionally marginalized communities. Better support and retention strategies for faculty of color are needed in academic programs and throughout institutions. There is still so much work to be done … Black Girl White Coat is just getting started.
Revolutionizing Information Access
Jaskirat Dhanoa, MD, PGY3; Nicholas Stark, MD, MBA, PGY4; Christopher Peabody, MD, MPH, University of California San Francisco, Department of Emergency Medicine, Acute Care Innovation Center

Dr. Dhanoa
Challenges presented by the COVID-19 pandemic pushed many emergency departments’ stagnant information distribution systems to a breaking point, requiring rapid adaptation to support a constantly changing clinical care environment. San Francisco General Hospital (SFGH), a University of California San Francisco-affiliated site, was no exception. As our emergency department became overloaded with rapidly-changing clinical information, the Acute Care Innovation Center (ACIC) set out to improve access to critical clinical information. The ACIC uniquely brought together a group of residents, hospital leadership, and medical students to account for different perspectives and tackle problems in an innovative manner. Our team learned that clinicians felt overwhelmed by the volume and speed of changing clinical information that was communicated from emails to cloud folder uploads. Clinicians did not know where to find the most up-to-date information. And text-heavy documents were difficult to apply in real-time on shift.

Dr. Stark
The design process led our team to an idea that was profound in its simplicity: democratizing information through an open-access, mobile-friendly, centralized digital information hub. Today, that idea has become an evolving clinical information platform called E*Drive.
E*Drive currently hosts a broad array of clinical information, ranging from COVID-19 guidelines to announcements to discharge resources, and it displays this information in a simple, standardized flow-chart style to enable in-the-moment utilization on shift. The platform has been profoundly successful, increasing access to clinical information in our emergency department by over 230 percent (from 0.13 views/day with the legacy system to nearly 30 views/day in September 2021), with 77 percent of clinicians reporting improved access to clinical information and 70 percent endorsing improved efficiency on shift as a result of E*Drive.

Dr. Peabody
Our team was able to build, launch, and sustain E*Drive for nearly free, all without in-depth tech experience. To do this, we built E*Drive on Drupal—our institution-supported web content management system—and utilized GoogleSlides to create the flow-chart style guidelines. E*Drive is easily accessible via a direct link in our medical record system or a short URL on any device with an internet connection. The platform layout is optimized for rapid information access with an average of three clicks from the homepage or via a robust search tool. The dynamic, modular nature of the E*Drive platform allows continued growth and evolution in response to user feedback. For example, we recently developed a first-of-its-kind Discharge Navigator tool (https://edrive.ucsf.edu/dcnav) that helps clinicians refer vulnerable patients to tailored community resources based on their demographics and needs. We also recently digitized frequently utilized forms, such as procedure consents, that previously needed to be accessed in cluttered filing cabinets.
E*Drive has revolutionized how our emergency department distributes and stores critical clinical information. By creating a system that is affordable, portable, and adaptable, our team hopes to inspire other emergency physicians including residents to develop similar innovations to accelerate guideline accessibility in the future.
Histories of our Present Illness
Luke Messac, MD, PhD, PGY4, Brown Emergency Medicine Residency

Dr. Messac
As a physician historian, I use techniques from history, anthropology, and epidemiology to study determinants of health outcomes. I completed my MD/PhD with a focus in the history of science, and have written about international opiate regulations, population control campaigns, economic indices, AIDS treatment activism, and hepatitis C diagnostic technologies. The aim of my research is to show how our way of delivering and paying for medical care developed, and how we might do better.
Today, I am studying the history of medical debt collection and the impact these debts are having on Americans’ lives. Since the 1980s, unpaid medical debts have moved from obligations negotiated by doctors and patients to financial instruments traded on impersonal financial exchanges. Spurred in part by cuts in public funding and insurance companies’ turn toward cost-sharing, hospitals have faced more bad debts. In response, health care institutions sent overdue bills to collection agencies and debt buyers. Divorced from the physicians’ bond to patients, debt collectors exercise draconian techniques, using wage garnishments, liens on homes, and lawsuits to extract profits from patients. Aggressive debt collection and third-party debt purchasing have continued to spread.
Another area of my research examines how health professionals respond to scarcity. My book, No More to Spend: Neglect and the Construction of Scarcity in Malawi’s History of Medicine, is a history of medical neglect in Malawi. Using the stories of doctors, patients, and political leaders, the book shows how colonial and postcolonial administrations used claims of scarcity to justify the dismal state of health care. Scarcity was not inevitable but was instead the product of choices by powerful actors to siphon financial resources away from medical care.
The COVID-19 pandemic highlighted the urgent need to study scarcity. New shortages have emerged, particularly in nursing staffing. This experience revealed the many tolls—psychological, economic, and clinical—exacted by not having enough resources to care for patients safely. In settings plagued by chronic scarcity, health care professionals face these inadequacies every day. Economists and psychologists have demonstrated how scarcity impairs the ability to make rational decisions. This has relevance to the practice of emergency medicine, particularly in low-income settings, where the constant pressure of not being able to practice the standard of care and the knowledge that one works in a system of tiered access can contribute to burnout, rushed diagnoses, and improper management. By understanding the pathophysiology of scarcity, we will improve outcomes and be better equipped to address health inequity.
 Dr. Borelli is an emergency medicine resident at the University of Texas Health San Antonio and ACEP Now resident fellow.
Dr. Borelli is an emergency medicine resident at the University of Texas Health San Antonio and ACEP Now resident fellow.
The Art in Medicine
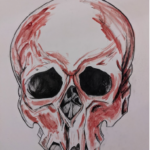 Cara Borelli, DO, ACEP Now Resident Fellow, recently interviewed Katrina Lettang, MD, for this month’s Resident Voice video. Dr. Lettang shares her experience working with various art mediums as a way to share personal experiences as an emergency physician through art. One painting features human blood to try and capture the duality of something doctors see every day.
Cara Borelli, DO, ACEP Now Resident Fellow, recently interviewed Katrina Lettang, MD, for this month’s Resident Voice video. Dr. Lettang shares her experience working with various art mediums as a way to share personal experiences as an emergency physician through art. One painting features human blood to try and capture the duality of something doctors see every day.
References
- Childhood surroundings matter more than genes for would-be inventors. The Economist. 2017(12).
- Smith N. Nurture Counts as Much as Nature in Success. Bloomberg Opinion. 2017(12).
Pages: 1 2 3 4 | Multi-Page




No Responses to “Emergency Medicine Residents Share Their Innovations in Our Field”