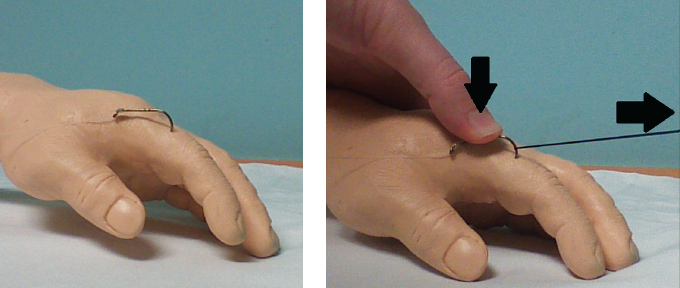
Figure 5. String yank technique.
The discussion of who receives prophylactic antibiotics remains controversial and is left up to the provider. If antibiotics are deemed necessary, doxycycline, trimethoprim-sulfamethoxazole, or fluoroquinolones are preferred for gram-negative coverage of organisms that are commonly found in recreational water-sport injuries. As a general rule of thumb in fishhook accidents, if the hook is embedded superficially, then there is no evidence to support prophylactic antibiotics. However, if the fishhook is embedded deeper or near neurovascular structures, then providers should consider prophylactic antibiotics, depending on the type of exposure (eg, saltwater versus fresh water; see Table 1). Stronger consideration for prophylaxis should also be made if the patient is immunocompromised.4

Table 1. Antibiotic Recommendations for Fishhook Injuries
*If the patient has an allergy to fluoroquinolone or doxycycline, use TMP-SMX as alternative coverage.
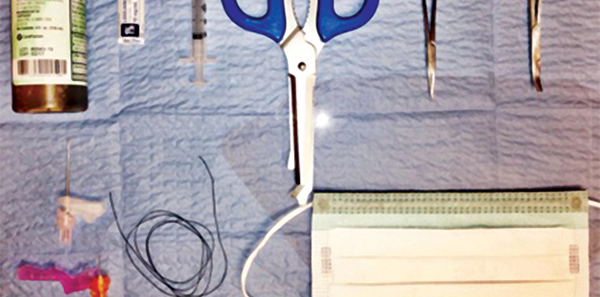
Equipment and Techniques (see Figure 1)4
- Povidone-iodine or chlorhexidine solution
- Local anesthetic solution without epinephrine
- 3 mL syringe
- Wire cutter
- Needle driver
- Hemostat
- 18-gauge needle
- 25-gauge needle
- String, fishing line, or 2-0 silk suture line, at least 50 cm in length
- Safety glasses, goggles, or a face mask with an eye shield for both the provider and patient
Proceed to cleanse the embedded area of debris, apply iodine or chlorhexidine solution, and allow the area to dry. Hooks with more than one point (eg, treble hooks) or lures/bait with more than one hook should have uninvolved points taped or cut off to prevent accidental embedding of uninvolved hooks while removing the embedded hook.5,6
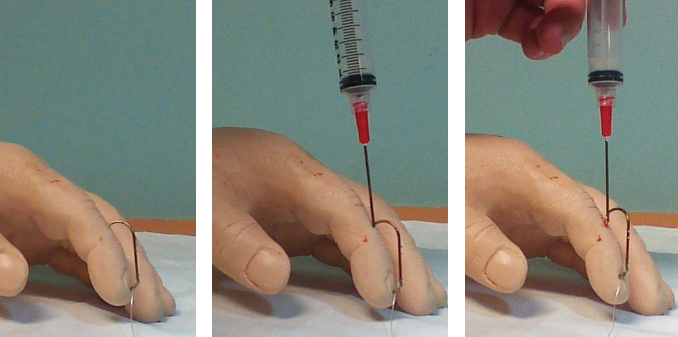
Pull through technique for single- and multi-barbed hooks (see Figures 2 and 3).
This is a great technique for large-caliber hooks with barb near the surface of the skin in the ears, nasal cartilages, or joints. Once preparation of site is complete, proceed to locate the barb end of the hook and inject 0.5–1 mL of local anesthetic (without epinephrine) over the embedded barb region. Allow a couple of minutes for full anesthetic effect. Proceed by grasping the shaft end of the hook with needle driver and advancing the hook until the last barbed section of the hook is exposed. Grasp the barbed section with a hemostat. If a single-barbed hook (barbed only at the hook tip) is embedded, use wire cutters to cut the hook proximally (toward the shaft end), and with the needle driver, pull back on the shaft and withdraw reverse of the direction of entry. If a multi-barbed hook is embedded or barbs are located on the shaft, advance the hook until the hook and barb are exposed. Grab this end with a hemostat. Use a wire cutter to cut the shaft, and without losing control of hemostat, pull the hook through (advancing toward the direction of entry).4
Pages: 1 2 3 4 | Single Page




No Responses to “Emergency Medicine Techniques, Equipment List for Removing Fishhooks Lodged in Patients”