Face-mask ventilation is considered a fundamental procedural skill in emergency medicine. We have historically deployed it when patients are apneic, are hypoventilating, or need assistance with oxygenation. We keep bag-mask units at the head of every bed in the emergency department.
Explore This Issue
ACEP Now: Vol 36 – No 01 – January 2017The world of airway management has evolved since the self-inflating bag-valve mask (BVM) was first created more than 50 years ago. In elective anesthesia, the laryngeal mask airway (LMA) has entirely replaced face-mask ventilation as a strategy for airway and anesthetic management in cases with a low risk of aspiration. In fact, the laryngeal mask is now used in the majority of elective anesthesia cases worldwide. It also has a rapidly growing presence in the world of prehospital care, especially in the United Kingdom and Europe.
The tip of the laryngeal mask wedges into the upper esophagus, behind the cricoid cartilage. It provides a wedge-shaped “stopper” to the upper esophagus; it’s not quite as effective as a tracheal tube in isolating the trachea from the esophagus but is far better than pushing gas by face mask into the shared upper aero-digestive tract of the pharynx.
LMA-type devices have replaced intubation and mask ventilation in elective anesthesia because they are better for both patients and operators. The laryngeal mask “sits” itself around the curve of the tongue and stays in position. The face mask requires continued downward pressure on the mask to maintain a seal. It can also be augmented by compressive head straps. The laryngeal mask can be easily used to bag a patient with one hand stabilizing the top of the device and the other squeezing the bag. This is not the case with a face mask. Holding the mask against the face works poorly, even with an “E-C grip” (using first and seconds digits [“C”] to hold the nasal bridge of the mask and the third, fourth, and fifth digits [“E”] to hold the lower mask).
Face-mask ventilation is as ergonomically smooth as walking in ski boots. The mask seals by being pushed onto the face, but this motion also pushes the mandible, base of the tongue, and epiglottis downward. And particularly in supine patients with no muscular tone, the base of the tongue, epiglottis, and mandible fall backward, causing “collapse” of the airway. Without continuous active lifting of the angle of the mandible, the airway obstructs. Conversely, the laryngeal mask seal is achieved by the same soft tissues falling backward onto the bowl of the device. It is not the inflation of a cuff that creates a mucosal seal; the newest and best laryngeal masks have, in fact, no cuffs at all. They mirror the laryngeal anatomy.
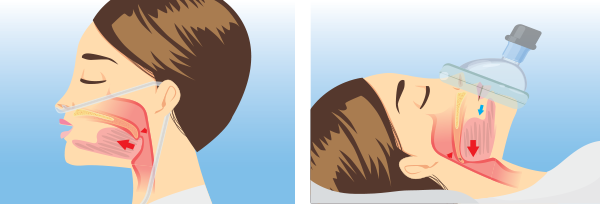
ILLUSTRATION: Chris Whissen & shutterstock.com
The laryngeal mask is, in fact, the only gravity-enhanced ventilation device. Gravity and loss of tone defeat the face mask. Conversely, administration of propofol, which induces a deep loss of upper-airway tone, is far and away the most commonly used medication for laryngeal mask anesthesia. The loss of tone in a supine position is ideal for creating the laryngeal mask seal around the bowl of the device. The soft tissues of the upper airway (base of tongue, epiglottis, and perilaryngeal structures) collapse backward onto the bowl of the LMA as muscular tone about the mandible is abolished.
In addition to the ergonomic challenges of doing effective mask ventilation—trying to create a face seal while pressing against the face but pulling up on the mandible simultaneously—there are many physiologic reasons why mask ventilation in a flat position is bad for oxygenation and also why it has a high risk for regurgitation. As a face mask is squeezed over the mouth, the oropharynx gets pressurized (see Figure 1). The goal is to have air only go into the lungs as opposed to the collapsed esophagus. Unfortunately, as pressure increases, especially at about 20 cmHg, air will enter the esophagus and subsequently the stomach. This insufflation of the stomach then leads to regurgitation of stomach contents back up the esophagus to the perilaryngeal area of the hypopharynx (at the top of the esophagus). Regurgitation risk is dramatically increased by having the patient’s stomach and head on the same level or, in an obese patient, the stomach higher than the mouth when the patient is supine. As the stomach gets insufflated, gravity promotes regurgitation of stomach contents into the upper airway.
The LMA, in contradistinction to a face mask, provides some isolation of the esophagus and larynx. The tip of an LMA-type device wedges into the upper esophagus. It’s not a complete isolation like a cuffed tube in the trachea, but by “corking” the top of the esophagus, there is some protection from gas entering the esophagus. Additionally, the bowl of the LMA is sitting directly under the laryngeal inlet, so the amount of pressure needed to get oxygen into the lungs is less than what is used typically with a face mask, having to start from outside the mouth and flow around the tongue.
In addition to the ergonomic difficulties of face-mask ventilation, problems creating an effective seal, and issues delivering oxygen into the lungs at low pressure, mask ventilation in a supine position has many disadvantages in terms of oxygenation.
In a flat position, the abdominal contents push the diaphragm upward, reducing the functional residual capacity of the lungs. Additionally, the posterior lung segments collapse.
Unlike pressurization of the oropharynx, pressurization of the nasopharynx causes passive opening of the airway as the soft palate is pushed away from the posterior pharynx (see Figure 1). Combining nasal oxygen with pulling on the mandible is an incredibly easy and fast way to open the upper airway. Oxygen shoots from the nasopharynx, down into the upper airway, and into the trachea. In the patient who is upright, the diaphragm drops and the lungs expand. Through the miracle of hemoglobin, oxygen is drawn down the trachea as it gets absorbed across the alveolar capillary membrane even without positive pressure ventilation (apneic oxygenation).
I used to bag patients as my initial response to hypoxemia in the emergency setting. Now, I put Oxygen On, Pull on the mandible, and Sit the patient up (OOPS). I have done this in the setting of oversedation and narcotic overdose, which resulted in complete apnea, and oxygenation improves quickly. I sometimes augment nasal oxygen at the top of the flow meter 15+ liters with a non-rebreather to boost oxygen flow >30 lpm.
In cardiac arrest, I used to bag patients while preparing to intubate. Now, I use passive apneic oxygenation and, if necessary, place an LMA-type device to run the initial portion of the code.
My current use of mask ventilation is only when I want to deliver some positive end-expiratory pressure (PEEP; PEEP valves should be on every BVM). This is generally only used when inducing patients for intubation. I gently ventilate for a couple of breaths when I use muscle relaxants to confirm that I can bag the patient and to expand the alveoli during the onset phase of muscle relaxants. I always do so in a head-elevated position (at least ear-to-sternal notch). I am careful to use low pressure, low volumes, and low rates, except in situations of compensatory respiratory alkalosis. My use of face-mask ventilation in these settings is generally with a nasal cannula, which helps stent the airway open and augment flow. I choose to perform face-mask ventilation in this situation, as opposed to an LMA, because I am worried about the LMA device being inserted too early, which could trigger active vomiting before rapid-sequence intubation medications kick in.
The role of face-mask ventilation in emergency situations is rapidly diminishing. I believe the first response to hypoxia should always be Os up the nose, either a standard nasal cannula combined with a non-rebreather to get flows >30 lpm or special high-flow, warm, humidified nasal cannula systems. Sit the patient upright as much as possible and pull on the mandible. In cardiac arrest, passive oxygenation and an LMA-type device should be used preferentially over bagging a patient in a flat position. If you have to use a face mask to provide PEEP (ie, BVM with a PEEP valve or continuous positive airway pressure mask), always do so in an upright position.
Pages: 1 2 3 4 | Multi-Page





3 Responses to “Should Emergency Physicians Abandon Face-Mask Ventilation?”
January 30, 2017
Jose Dionisio Torres, Jr., MDWhat do we have is cost and demand? And the illusion of patient safety.
The public doesn’t know the difference from a bvm..and and lma/or king lt.
These devices are better in ventilation than bvm. But need the bvm if there is a contraindication.
Facemask cheaper but ensures air will go into the stomach ensuring higher risk of aspiration. But don’t use in Coffin position described by you Dr. Levitan. Ramp them up as high as possible if bvm is to be used.
Thank you for the Post Dr. Levitan.
Thank you Mr. Robert Ackerman on sharing this post with me.
March 5, 2017
Craig NavarijoI believe the bvm can be made much more safely than it is today…
in fact, I have working protoypes of a bvm that an individual can selectivley limit volume delivery with.
and that makes maintaining a seal extremely easy ….
March 6, 2017
Steve LeCroyDr. Levitan,
Would you consider using one or two NPA’s like naso-flo that can provide supplemental oxygen along with CPAP instead of a cannula and non-rebreather mask?