
An excerpt from our Medical Editor in Chief Dr. Cedric Dark : As you read our August issue, may also notice a theme emerging from some of the other pieces in this issue: they touch on controversial issues. This is both a symptom and side-effect of our current social, political, and professional climate. The topics discussed in this issue are meant to highlight the work, and the worries, of our profession. No matter which side you take, each topic affects us all professionally and personally. Our diversity of experience and opinion is what makes emergency medicine, the American College of Emergency Physicians, and America itself enriching. I hope that you will enjoy reading this issue, and most of all, learn something new from what you find inside.
Explore This Issue
ACEP Now: Vol 41 – No 08 – August 2022Violence in the emergency department (ED) is nothing new. A 2005 study showed that between 35–80 percent of hospital staff have been physically assaulted at least once during their careers.1
COVID-19 may have also exacerbated an already existing truth. In November 2021, a survey conducted by the National Nurses United and the Surgeon General indicated eight out of 10 health care workers experienced at least one type of workplace violence during the pandemic, with two-thirds having been verbally threatened, and one-third of nurses reporting an increase in violence compared to the previous year.2 Patients in emergency departments sometimes have violent outbursts; some of these patients have access to weapons—either prefabricated or improvised. In 2020, ACEP Now published statistics surrounding firearms in the ED, revealing that almost 60 percent of health care professionals working in American EDs encountered firearms in or near the ED at least once per year.3 Recent mass shootings, inside and outside the hospital, have directly impacted emergency physicians—either as caregivers or as victims—and reignited the debate over the wisdom of concealed carry in the emergency department.
But a recent slew of gun violence in the ED has prompted debate on the efficacy of workplace safety. In 2016, Parrish Medical Center in Florida experienced an active shooter who shot and killed a 92-year-old patient and her caregiver.4 In 2021, a hostage situation at the Children’s Medical Group in Austin, Texas, left two physicians dead, including the gunman.5 In June, EMS workers in Conroe, Texas, were nearly injured after disarming a patient who fired shots in the emergency department.6
Also in June, the murders of Preston J. Phillips, MD, FAAOS, an orthopedic surgeon, and Stephanie J. Husen, DO, a sports medicine physician, along with two other people by a disgruntled patient at a hospital in Tulsa, Oklahoma, highlighted the dangers posed to health care workers—dangers which ED staff know all too well.7
Firsthand Encounters and Experiences

Dr Marco
Catherine A. Marco, MD, FACEP, encountered an active shooter the same day as the Tulsa, Oklahoma, mass shooting.8 On June 1, her hospital in Ohio experienced an active shooter incident ending with both the patient and security guard dying. “I was just working a regular shift with the residents and we had a full emergency department. We were boarding a lot of patients. Someone came running from triage yelling, ‘There’s an active shooter out in triage.’ And this brought to mind the fact that all the training in the world might not help.”
The shooter was a prisoner in the custody of law enforcement and had been admitted, waiting for a hospital bed. “He had been in the ED for many hours without any incident,” Dr. Marco recalled. “Somehow [he] got the security officer’s weapon, shot the security officer, ran out to the ED parking lot, and shot himself. And they were both killed. We attempted resuscitation on both of them, but neither one could be resuscitated.”
Dr. Marco served on the reference committee during the ACEP Council Meeting in Boston, Massachusetts, in October 2021 where a proposal to turn the ED into a firearm free zone was put forth. “Resolution 32: Firearm Ban in EDs Excluding Active Duty Law Enforcement” was also formally supported by the Vermont Chapter ACEP, the American Association of Women Emergency Physicians Section, and ACEP’s Diversity, Inclusion and Health Equity Section. Read the sidebar on page 7 to retrace the path of 2021 Council resolution 32 from proposal to policy.

Dr. Kozak
Paul Kozak, MD, FACEP, an emergency physician in Arizona, served alongside Dr. Marco on the reference committee that analyzed Resolution 32. He, too, has had several encounters with ED violence. “I’m aware of about three episodes of people drawing guns in a hospital, and most of them were domestic disputes or in the offices of disgruntled patients,” explained Dr. Kozak. “Over my career, many times I have stood up and in between a patient and a nurse, when the patient got violent toward a nurse. It’s a pretty common occurrence.”

Dr. Thran
Resolution 32 cosponsor Niki Thran, MD, FACEP, who is also chapter President of Vermont ACEP and Democratic candidate for U.S. Senate, explained her position as, “I am against anyone carrying firearms in the ED with the exception of on-duty law enforcement, including federal agents and military police,” she said. “Hospital security too, if they are hired as such. I definitely do not think physicians and other staff should be carrying firearms in the ED.”

Dr. Hsu
Tony Hsu, MD, is an emergency physician in Ann Arbor, Michigan. As chair of ACEP’s Public Health & Injury Prevention Committee, he led the group assigned to translate aspects of Resolution 32 into ACEP policy. “I don’t think as on duty physicians we should have to deal with our own concerns of penetrating injury. I like to have specialists when I have a trauma patient coming in. I want to have a specialist when somebody else has a firearm and perhaps maybe threatening others,” explained Dr. Hsu. “When we think about violence in the ED, the ones who bring guns into the workplace should be safety personnel … that made me want to update the policy.”

Dr. Phillips
James Phillips, MD, an emergency physician, associate professor, and chief of disaster medicine at George Washington University, served as a tactical physician for a number of years, and is active in ACEP’s sections focused on disaster and tactical medicine. “We still don’t have protections in our emergency departments that we need and for anyone that doubts that, look at the debate we’re having right now that emergency physicians feel that they need to carry weapons to protect themselves,” Dr. Phillips said.
Gun Ownership Among Emergency Physicians

Dr. Gasper
Not all emergency physicians share Dr. Thran’s viewpoint on restricting the carrying of firearms in the ED. A large minority of emergency physicians, 43 percent, own firearms, according to a study published in 2021.9 Among them is Steve Gasper, MD, who currently works in Dallas, Texas, and did an elective in tactical medicine during residency. Before that, Dr. Gasper served as a forward observer and a designated marksman in the U.S. Marine Corps. “I think there’s a tendency to have a boiler plate of, ‘No, [guns are] not allowed. Just call the police,’” Dr. Gasper said. “It’s kind of wishful thinking to say, ‘Well, we’ll just make it a gun-free zone and that’ll solve the problem.’ But that really doesn’t. I mean, most of the mass shootings occur in gun-free areas.”

Dr. Coppola
Marco Coppola, DO, FACEP*, has been in the military for 37 years and is the chief of medical staff at The Colony ER Hospital in The Colony, Texas. “I think every emergency department should have active shooter drills. Just like we practice a disaster drill, every emergency department should do that,” he explained. Dr. Coppola served as chair of the ACEP task force to rewrite the ACEP Firearms and Injury Prevention Policy in 2013. “We thought it was very important not to legislate and not to contradict existing laws. What was interesting is that [at the time] we tried to come up with the most comprehensive firearm policy possible.”
When asked about his personal belief on firearms in the emergency department, Dr. Coppola said, “I firmly believe that it is every person’s right to defend themselves. If you’re in a remote part of the ED where there is very little security or security is all on the other side and a patient becomes violent and you have no way to protect yourself, how do you do that? You could call for help, but you might be dead by the time they come.”
Rural Considerations
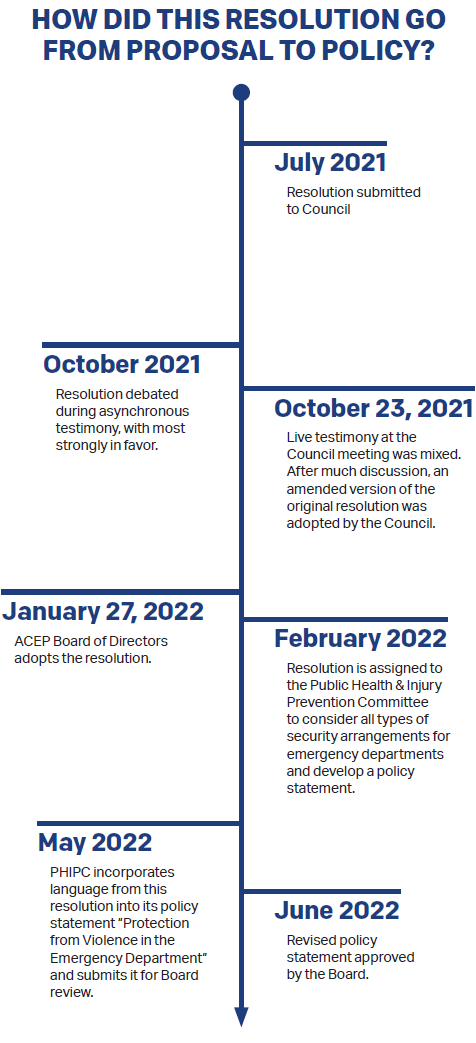
At its 2021 meeting, the ACEP Council passed Resolution 32: Firearm Ban in EDs Excluding Active Duty Law Enforcement, after extensive discussion. The majority of the debate on the Council floor was surrounding the first Resolved clause: “That ACEP promote and endorse that Emergency Departments become “Firearm Free” Zones, with the exception of active duty law enforcement officers, hospital security, military police and federal agents.”
(Did you know you can check on the status of recent Council resolutions? Visit acep.org/actions-on-council-resolutions to do a deeper dive. The archive goes back to 1993.)
Unlike many urban emergency departments, many rural emergency departments do not have armed security guards. “Do I carry when I’m not at work? Yes, I do,” says Edwin Leap, MD, who works in small and medium-sized emergency departments in southern Appalachia. “I believe that concealed carry is a reasonable thing, but I don’t do it in the hospital. Now, having said that, I’ve worked in lots of places that had little to no security. In fact, I worked once in a small town in Kentucky. There was a critical access hospital and after 5 p.m., the city police closed up, they weren’t available, and the only person available was the highway patrolman who had responsibility for that area. And that person might have three or four counties. So, when emergency physicians feel like they’d like to carry at work, I’m sympathetic. I understand.”
Dr. Marco, who personally does not feel that physicians should be armed while on duty, cites the violent confrontation in her own ED as one that demonstrates how complicated the issue can be. “[Ours was] a situation though, where any amount of gun control or weapon screening would not have helped because it was a security officer’s weapon.” Evidence shows that 23 percent of firearm attacks in the ED occur after the assailant takes a weapon from a law enforcement officer.10 “I think we all agree that security officers should be armed,” Dr. Marco said.
Research indicates that carrying a firearm may increase a victim’s risk of injury when a crime is committed, with one study indicating that people in possession of a gun may be more than four times more likely to be shot in an assault.10 An FBI analysis of 160 active shooter incidents from 2000–2013 found that active shooter incidents were rarely stopped by armed individuals who were not law enforcement returning fire.11 In fact, four times as many shootings were stopped by unarmed civilians restraining the shooter. A 2015 Harvard University study analyzed data from 2007 to 2011 found that of more than 14,000 crimes in which a victim was present, just under one percent involved a gun used in self-defense. The Harvard Injury Control Research Center also found that self-defense gun use is, “rare and not more effective at preventing injury than other protective actions.”12
What About Resolution 32?
After lively discussion during the 2021 Council Meeting in Boston, Resolution 32 eventually passed and was adopted by ACEP’s Board of Directors on Oct. 2021. The result of this vociferous debate is for now settled in an ACEP Policy Statement, “Protection from Violence in the Emergency Department,” which was revised to address Resolution 32. The policy statement’s list of hospital and administrative responsibilities to ensure the safety and security of the ED now includes these two items:
- Erect signage and provide for appropriate securing of firearms outside of the ED, designating the ED a ’Firearm-Free Zone.’
- Coordinate the health care institution’s security system with local law enforcement agencies when developing policies for safekeeping of firearms; trained and on-duty law enforcement officers, hospital security, military police, and federal agents may be acceptable exceptions to the ’Firearm-Free Zone.’
ACEP’s policy statements are available to view in full at acep.org/policystatements.
 Danielle Galian (@Danielle_Galian) is editor of ACEP Now.
Danielle Galian (@Danielle_Galian) is editor of ACEP Now.
References
- Clements, TP, et al. Workplace violence and corporate policy for health care settings. Nursing Economics website. Available at: http://www.ncdsv.org/images/WorkplaceViolenceCorporatePolicyHealthCare.pdf. Accessed July 20, 2022.
- Workplace violence and covid-19 in health care how the hospital industry created an occupational syndemic. National Nurses United website. Available at: https://www.nationalnursesunited.org/sites/default/files/nnu/documents/1121_WPV_HS_Survey_Report_FINAL.pdf. Accessed July 20, 2022.
- By the numbers: firearms in the emergency department. ACEP Now. 2020;39(11):6.
- Minemyer P. Hospital Shooting: Florida Facilities Beef up Security with Armed Guards, Random Bag Checks. Fierce Healthcare website. Available at https://www.fiercehealthcare.com/hospitals/florida-hospitals-take-a-look-at-security-after-deadly-shooting. Accessed July 20, 2022.
- Autullo R, Plohetski T. Hostages say Naurmanchi targeted doctors in standoff that killed beloved Austin pediatrician. Statesman website. Available at https://www.statesman.com/story/news/2021/01/27/doctorlindley-dodson-killed-austin-hostage-situation-shooting-bharat-narumanchi/4277191001/. Accessed July 20, 2022.
- Texas EMS provider disarms patient after shots fired inside hospital. EMS1 website. Available at: https://www.ems1.com/shooting/articles/texas-ems-providerdisarms-patient-after-shots-fired-inside-hospital-PdjhenJUkOUMKxdP/. Accessed July 20, 2022.
- Ketterer AR, Ray K, Grossestreuer A, et al. Emergency physicians‘ familiarity with the safe handling of firearms. West J Emerg Med. 2019;20(1):170–176.
- Spicker K, Perry P. Police: Shooter ran through Miami Valley Hospital, pointed gun at others. Dayton Daily News website. Available at: https://www.daytondailynews.com/crime/large-struggle-took-place-prior-to-shooting-at-miami-valley-hospital/JJJFYAI7NZDNXKT57GTC3SXDUQ/. Accessed July 20, 2022.
- Farcy DA, Doria N, Moreno-Walton L, et al. Emergency physician survey on firearm injury prevention: Where can we improve? West J Emerg Med. 2021;22(2):257–265.
- Branas CC, Richmond TS, Culhane DP, et al. Investigating the link between gun possession and gun assault. Am J Public Health. 2009;99(11):2034–40.
- A study of active shooter incidents in the United States between 2000 and 2013. FBI website. Available at: https://www.fbi.gov/file-repository/active-shooter-study-2000-2013-1.pdf/view. Accessed July 20, 2022.
- Gun threats and self-defense gun use. Harvard Injury Control Research Center website. Available at: https://www.hsph.harvard.edu/hicrc/firearms-research/gun-threats-and-self-defense-gun-use-2/. Accessed July 20, 2022.
*The views and opinions expressed by Dr. Coppola are his own and do not necessarily reflect the opinions, views, or official policies of Nutex Health, Inc or any of its affiliates or associates, the Texas Military Department, or the Texas State Guard. Any content provided is not meant to malign any religion, ethnic group, club, organization, company, individual or anyone or anything else.




2 Responses to “Firearms and Emergency Department Safety”
August 20, 2022
Robert Hansen“Erect signage and provide for appropriate securing of firearms outside of the ED, designating the ED a ’Firearm-Free Zone”.
Truly one of the most useless ideas ACEP has ever come up with. Does anyone actually think “gun free zone” signs have EVER done anything to deter someone who wishes to cause harm on others? Schools are “gun free zones” and we see how well that works. It’s ridiculous to think that this will do anything to improve the safety of those of us who work in the ED.
August 21, 2022
Mike Magoon MD FACEPHospitals have always been “firearm free zones.” It is illegal to carry a firearm in the hospital – and the ED is part of the hospital. This ACEP policy seems redundant, and unfortunately accomplishes nothing. Evil people have never cared whether there is a sign on the door asking them not to bring weapons.
This policy only makes it more difficult for emergency physicians to carry a side arm, if they feel their welfare could be at risk in a rough ED.