
Acute agitation in children in the emergency department (ED) can be hazardous and distressing to patients, families and the ED team.1,2 Over 79 pediatric deaths have been attributed to restraint-related events in the U.S.3,4,5 It is important for the care of acute agitation to be safe, proactive, effective and patient-centered to ensure the well-being of the child, caregivers and ED staff. The federally funded Emergency Medical Services for Children Innovation and Improvement Center (EIIC) has partnered with experts from ACEP to develop and collate resources into a comprehensive Pediatric Education and Advocacy Kit (PEAK) on agitation.6 In this article, we will review the initial approach and management of acute agitation in children.
Explore This Issue
ACEP Now: Vol 41 – No 11 – November 2022Initial Assessment
Ensuring safety: The first step in the management of agitation is to ensure the safety of the patient, caregiver(s), and ED staff. Belongings should be removed, and when safe to do so the patient should be changed into a gown to confirm there are no items or substances on the patient that might cause harm. A checklist may assist in ensuring the removal of items.7 When available, the patient should be placed in a designated area dedicated to the treatment of patients with behavioral conditions, also known as a safe room.8 An appropriate level of observation should be initiated, including trained observers or security if needed.
Identification of etiology: Next, a focused history and physical examination to determine the etiology of the child’s agitation and any underlying risk factors is important. Potential etiologies include delirium, defined as a waxing and waning mental status associated with an underlying medical problem (i.e., metabolic, neurologic, traumatic, hypoxic, or infectious), substance ingestion or inhalation (intoxication, poisoning, or withdrawal), or acute underlying mental or behavioral condition (bipolar disorder, schizophrenia or psychosis). In addition, conditions that cause pain may lead to agitation, particularly among patients with autism spectrum disorder, communication disorders and/or developmental delay. For these patients, a careful history and examination may reveal causes of pain such as acute otitis media, pharyngitis, dental abscess, urinary tract infection, or constipation. Treating these underlying issues may address the agitation.
Initial Approach to the Child with Agitation
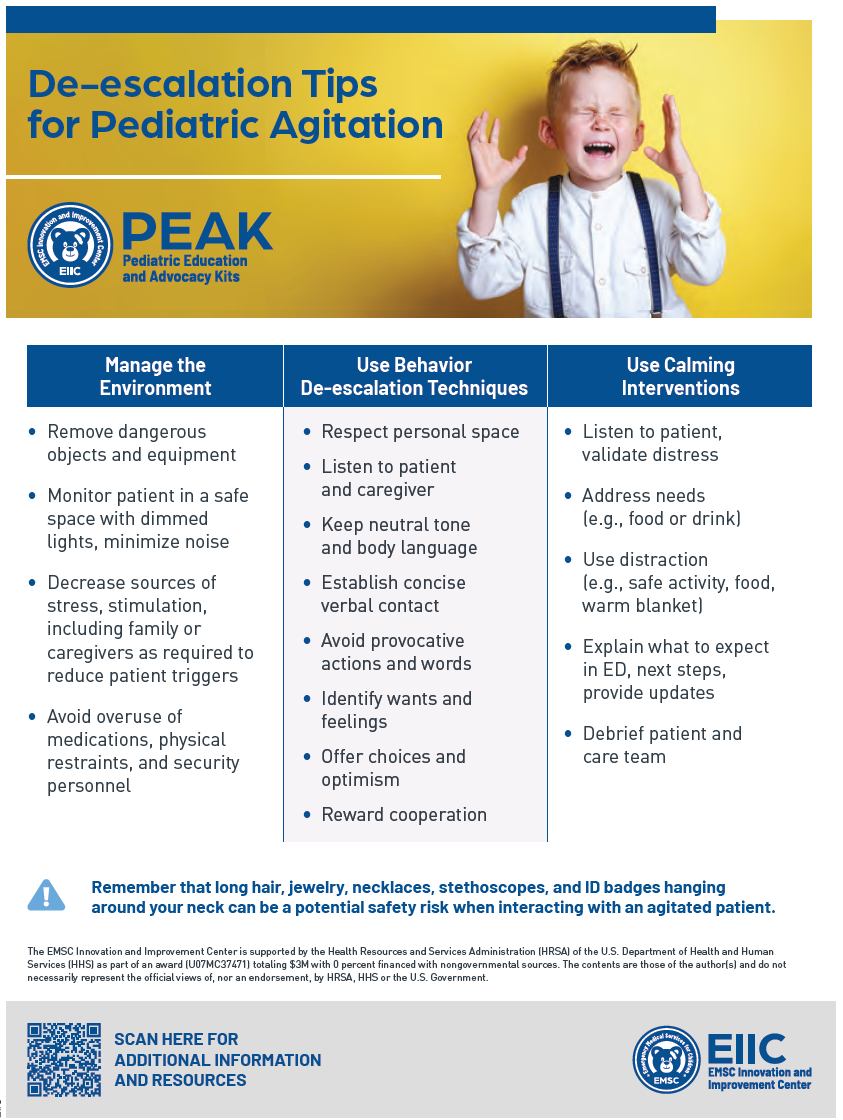
Figure 1. A de-escalation checklist for pediatric agitation. (Click to enlarge.)
Verbal de-escalation: Early use of verbal de-escalation techniques can be an effective means of resolving agitation swiftly. It is important to respect the patient’s personal space and maintain a calm behavior, facial expression, and posture (Figure 1). When possible, offer the child choices and positively reward cooperation. Additionally, consider a child’s developmental level and preferred means of communication, and provide instructions one step at a time (allowing the child time to process the information and respond). Triggers for agitation and successful de-escalation strategies should be recorded and communicated between team members during care transitions and can be assessed on initial intake of the patient.
Pages: 1 2 3 | Single Page



No Responses to “How to Manage Acute Agitation in Children”