
Acute agitation in children in the emergency department (ED) can be hazardous and distressing to patients, families and the ED team.1,2 Over 79 pediatric deaths have been attributed to restraint-related events in the U.S.3,4,5 It is important for the care of acute agitation to be safe, proactive, effective and patient-centered to ensure the well-being of the child, caregivers and ED staff. The federally funded Emergency Medical Services for Children Innovation and Improvement Center (EIIC) has partnered with experts from ACEP to develop and collate resources into a comprehensive Pediatric Education and Advocacy Kit (PEAK) on agitation.6 In this article, we will review the initial approach and management of acute agitation in children.
Explore This Issue
ACEP Now: Vol 41 – No 11 – November 2022Initial Assessment
Ensuring safety: The first step in the management of agitation is to ensure the safety of the patient, caregiver(s), and ED staff. Belongings should be removed, and when safe to do so the patient should be changed into a gown to confirm there are no items or substances on the patient that might cause harm. A checklist may assist in ensuring the removal of items.7 When available, the patient should be placed in a designated area dedicated to the treatment of patients with behavioral conditions, also known as a safe room.8 An appropriate level of observation should be initiated, including trained observers or security if needed.
Identification of etiology: Next, a focused history and physical examination to determine the etiology of the child’s agitation and any underlying risk factors is important. Potential etiologies include delirium, defined as a waxing and waning mental status associated with an underlying medical problem (i.e., metabolic, neurologic, traumatic, hypoxic, or infectious), substance ingestion or inhalation (intoxication, poisoning, or withdrawal), or acute underlying mental or behavioral condition (bipolar disorder, schizophrenia or psychosis). In addition, conditions that cause pain may lead to agitation, particularly among patients with autism spectrum disorder, communication disorders and/or developmental delay. For these patients, a careful history and examination may reveal causes of pain such as acute otitis media, pharyngitis, dental abscess, urinary tract infection, or constipation. Treating these underlying issues may address the agitation.
Initial Approach to the Child with Agitation
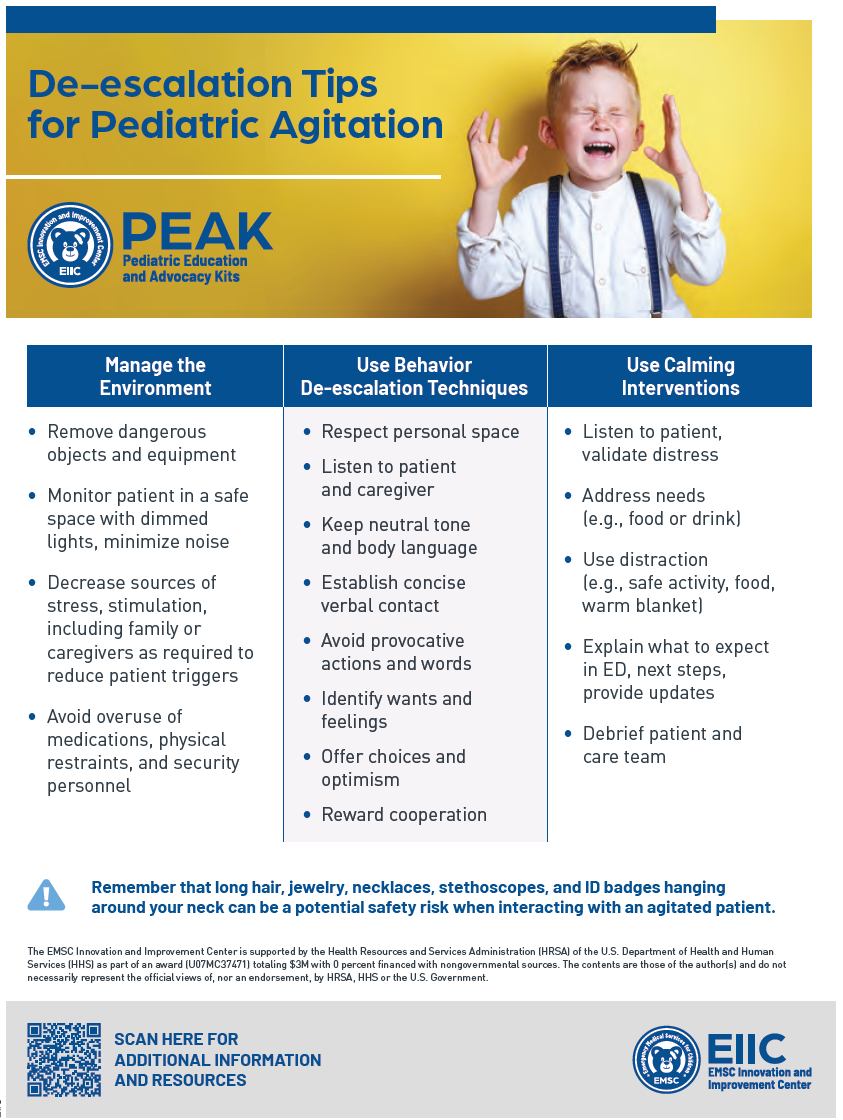
Figure 1. A de-escalation checklist for pediatric agitation. (Click to enlarge.)
Verbal de-escalation: Early use of verbal de-escalation techniques can be an effective means of resolving agitation swiftly. It is important to respect the patient’s personal space and maintain a calm behavior, facial expression, and posture (Figure 1). When possible, offer the child choices and positively reward cooperation. Additionally, consider a child’s developmental level and preferred means of communication, and provide instructions one step at a time (allowing the child time to process the information and respond). Triggers for agitation and successful de-escalation strategies should be recorded and communicated between team members during care transitions and can be assessed on initial intake of the patient.
Environmental modification: These strategies include dimming lights, reducing noise, removing potentially dangerous equipment, and minimizing staff presence when safe to do so (Figure 1).
Calming interventions: Consider using distraction with activities and breathing exercises appropriate for age and development.7 Children with autism spectrum disorder may benefit from soothing sensory items and visuals for communication.
Further Management
Pharmacologic treatment: Pharmacologic treatment may be indicated to manage severe agitation when verbal de-escalation fails or when patient or staff safety is at risk. In children, current practice is based on limited available research, extrapolation from the adult literature, and the consensus of experts.1,2 Several medication classes are available for managing agitation in children, including antihistamines, benzodiazepines, and antipsychotics.2 The primary pharmacologic consideration should be based on etiology and severity of the child’s agitation.2 If the patient has an existing scheduled home medication that is effective, the physician may consider administering the medication earlier than scheduled.
Use of physical restraint: Physical restraints should be applied as a last resort when needed to ensure the safety of the patient or staff. The preferred patient position for physical restraint is supine without pressure placed on the patient’s head or neck.4 Frequent reassessments should be performed to monitor the patient’s alertness, respiratory status, circulation, and level of agitation. Physical restraints should be removed as soon as it is safe to do so. It is important for physicians to acquaint themselves with regulatory requirements and jurisdiction-specific laws associated with the application of physical restraints in their area.1
Conclusion
Acute agitation in a child in the ED can be a potentially dangerous experience for the child, caregiver(s), and ED staff. Priorities for agitation care in the ED include the establishment of safety, assessment of the etiology of the agitation episode, utilization of effective de-escalation techniques, selection of medication when indicated, and monitoring after an episode of agitation. Visit https://bit.ly/PEAKAgitation to access the EIIC PEAK, which includes a variety of resource types and formats, from bottom-line recommendations and learning modules to podcasts and webinars. All resources are free and open access.
Dr. Foster is an instructor at Massachusetts General Hospital in Boston, Mass.
Dr. Li is assistant professor at Boston Children’s Hospital in Boston, Mass.
Dr. Hoffmann is assistant professor at Lurie Children’s Hospital in Chicago, Ill.
References
- Hoffmann JA, Pergjika A, Konicek CE, Reynolds SL. Pharmacologic management of acute agitation in youth in the emergency department. Pediatr Emerg Care. 2021;37(8):417-422.
- Gerson R, Malas N, Feuer V, et al. Pediatric best practices for evaluation and treatment of agitated patients (BETA) guidelines for management of acute agitation in children and adolescents in the emergency department: consensus statement of the American Association for Emergency Psychiatry. West J Emerg Med. 2019;20(2):409-418.
- Weiss EM. Deadly restraint: A Hartford Courant investigative report. Hartford Courant. October 11, 1998: A1.
- Chun TH, Katz ER, Duffy SJ, Gerson RS. Challenges of managing pediatric mental health crises in the emergency department. Child and Adolescent Psychiatric Clinics of North America. 2015;24(1):21-40.
- Nunno MA, McCabe LA, Izzo CV, et al. A 26-year study of restraint fatalities among children and adolescents in the United States: A failure of organizational structures and processes. Child and Youth Care Forum. 2022;51:661-680.
- EMSC Innovation and Improvement Center. Pediatric emergency & advocacy kits (PEAK). EICC website. https://emscimprovement.center/education-and-resources/peak/pediatric-agitation. Updated August, 2022. Accessed October 6, 2022.
- EMSC Innovation and Improvement Center. New England Regional Behavioral Health Toolkit. EICC website. https://emscimprovement.center/state-organizations/new-england/new-england-behavioral-health-toolkit. Accessed October 6, 2022.
- The Joint Commission. Ligature and/or suicide risk reduction – emergency department – safe rooms (designated spaces): FAQ. The Joint Commission website. https://www.jointcommission.org/standards/standard-faqs/hospital-and-hospital-clinics/national-patient-safety-goals-npsg/000002196/. Published June 27, 2018. Updated February 1, 2022. Accessed October 6, 2022.
Pages: 1 2 3 | Multi-Page



No Responses to “How to Manage Acute Agitation in Children”