The erector spinae plane block (ESPB) is a relatively new block, first described in 2016 as an analgesic technique for neuropathic thoracic pain.1 Since that time, this simple and safe technique has been adopted with enthusiasm and used with great efficacy to treat pain resulting from a wide array of pathological processes. Often referred to as the “poor man’s epidural,” the beauty of this single-injection high-volume block lies in its capacity to anesthetize the majority of the hemithorax. Additionally, the sonoanatomy of the ESPB is relatively simple and safe. Under the erector spinae muscles lie the transverse processes, which act as a bony “backstop” to prevent inadvertent puncture of any critical structures.
Explore This Issue
ACEP Now: Vol 40 – No 09 – September 2021Early uses of the ESPB were for neuropathic chest wall pain, breast surgery, and rib fractures.1–3 Furthermore, the ESPB was found to be particularly efficacious for posterior rib fractures that are typically not amenable to other approaches to thoracic analgesia (ie, the serratus anterior plane block).4 Early case reports have also shown that the ESPB can be applied to lumbar and sacral levels with similar efficacy for abdominal and pelvic pain.5,6 Most notably, some postulate that the ESPB may block sympathetic fibers (in addition to dorsal and ventral rami), thereby relieving visceral pain.7 This would explain a number of studies and case reports that suggest the ESPB may be effective in treating pain associated with visceral thoracoabdominal pathology, including renal colic, pancreatitis, and even appendicitis.8–10 The versatility and simplicity of the ESPB make it a highly useful technique for any emergency physician.
(click to enlarge)
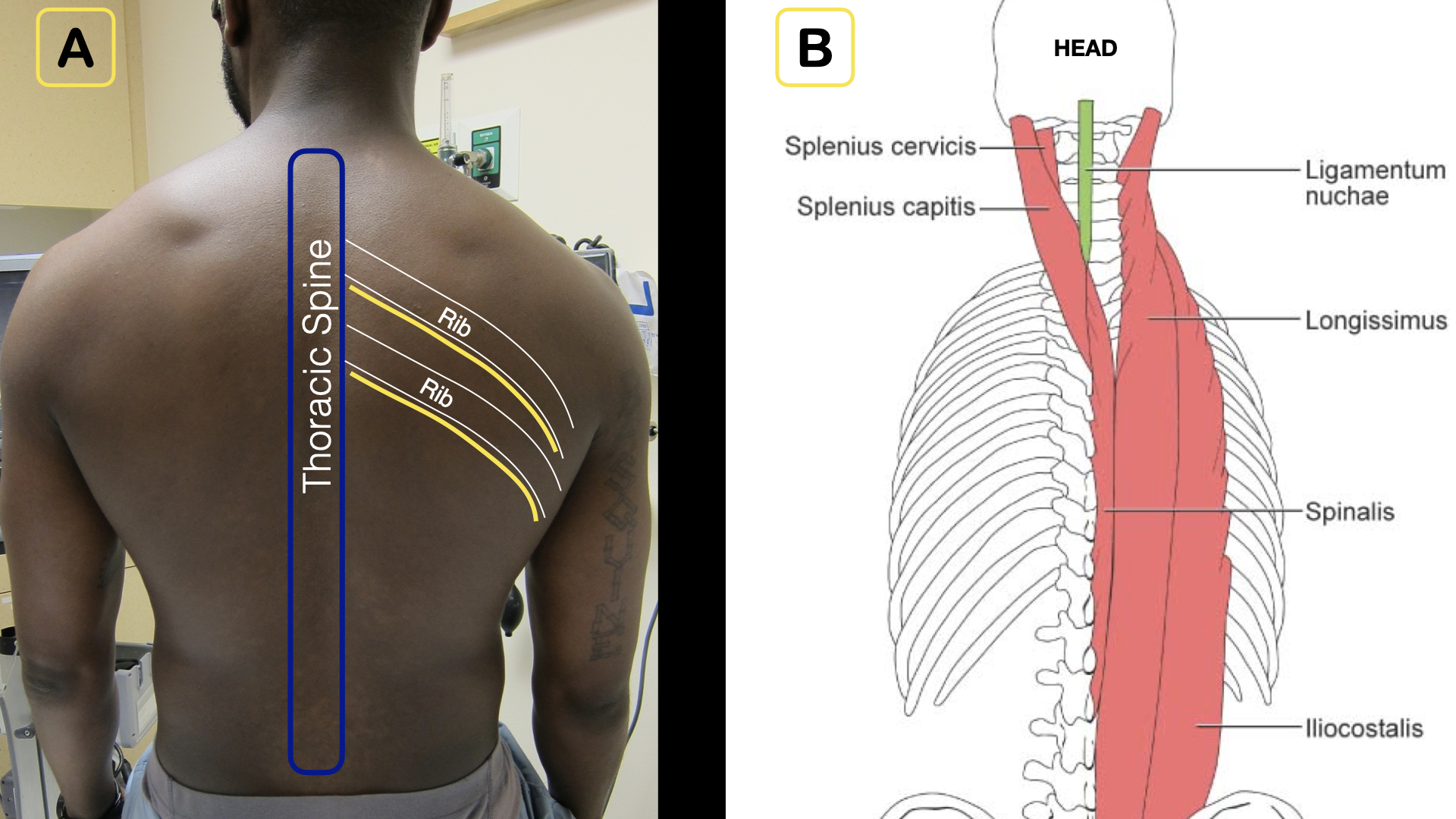
1A) Note the relationship of the thoracic spine, ribs, and intercostal nerves (yellow line).
1B) The erector spinae muscles lie just on top of the spine, forming an ideal target for deposition of anesthetic.
Credit: Arun Nagdev
Anatomy and Innervation
The erector spinae muscles run craniocaudally over the transverse processes, deep in the posterior chest wall (see Figure 1). The ESPB targets this fascial plane and anesthetizes the dorsal rami in addition to the ventral rami and proximal intercostal nerves (see Figure 2). As a result, the ESPB may be able to provide analgesia for the entire hemithorax. The ESPB is a planar block—or more simply, instead of targeting a specific nerve, the goal is to place anesthetic in a defined myofascial plane. Injectate spreads craniocaudally within the fascial plane, permitting analgesia for six to eight rib levels with a single high-volume injection of local anesthetic combined with normal saline flushes (between 20 and 40 mL). The erector spinae fascial plane extends inferiorly into the lumbar and sacral regions as well. Placement location of the ESPB can be adjusted to target the specific spinal levels associated with the painful pathology (eg, injection at T8 is used for pain associated with renal colic).8
Pages: 1 2 3 4 | Single Page


No Responses to “How to Perform an Erector Spinae Plane Block”