Unlike traditional awake flexible endoscopy, VAFEI can be performed very rapidly, which allows the procedure to be incorporated into an RSI-based paralyzed approach. RSI maximizes the likelihood of first pass success and for decades has been used in the majority of emergency department intubations.12,13,14,15
Explore This Issue
ACEP Now: Vol 41 – No 11 – November 2022VAFEI can be used as part of a topically anesthetized awake approach, however achieving sufficient local anesthesia that an awake patient will tolerate laryngoscopy requires more time than is available in many emergency intubation cases and is enabled by specialized equipment (e.g., atomizers, concentrated lidocaine) that may not be available.
VAFEI can also be incorporated into a ketamine-only strategy that attempts to take advantage of the safety benefit of ATI by maintaining spontaneous respirations while overcoming the challenges in executing effective topicalization, by using enough ketamine that the patient will tolerate laryngoscopy and tracheal intubation.16 The use of atomized lidocaine about the posterior oropharynx and glottis is still recommended, if feasible, to attenuate airway reflexes and laryngospasm that may impede tube delivery even in dissociated patients.
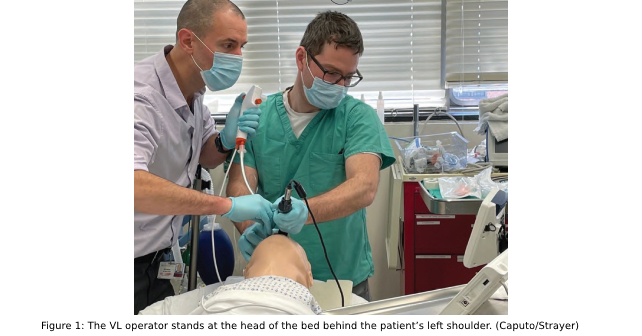
The primary drawback of the VAFEI technique is that it requires two operators: one to perform video laryngoscopy and one to advance the flexible endoscope. However, both operators need not be physicians, and in fact one operator can perform VAFEI by first completing laryngoscopy and then handing off the VL to an assistant positioned to the operator’s left, behind the patient. VAFEI requires that both VL and FE devices be available and ready, which is a barrier in many departments; however, the emergence of single-use, disposable VL blades and endoscopes allows wider adoption of this technology in emergency settings. Operation of the flexible endoscope in VAFEI does not require the same degree of skill as is needed to perform conventional flexible endoscopic intubation, but does require familiarity with the device and its basic functions, which can easily be acquired in a simulation training session.
Conclusion
VAFEI is a powerful intubation technique that takes advantage of the strengths of video laryngoscopy and flexible endoscopy while diminishing their drawbacks.17 It can be incorporated into approaches that preserve spontaneous ventilation and performed quickly enough to be used with paralysis and rapid sequence intubation. Because most anatomically difficult airways are unpredicted, it is essential that airway management strategies plan for first-attempt failure.18,19,20
Dr. Strayer is an emergency physician at Maimonides Medical Center, in Brooklyn.
Dr. Caputo is associate chief of the Department of Emergency Medicine at NYC H+H/Lincoln Medical Center in the South Bronx.
Pages: 1 2 3 4 5 | Single Page




No Responses to “How To Use Video-Assisted Flexible Endoscopic Intubation”