We read with interest the recent pro/con debate in ACEP Now (July 2016) about gun control. This debate followed reporting of advocacy for the restoration of federal funding for gun violence research in June by ACEP President Jay Kaplan, MD, and by the American Medical Association (AMA) (ACEP Now, June 2016). The July article purported to debate the merits of political advocacy for gun control by our profession. However, it confused legal advocacy with science advocacy, and so it perpetuates the misconception that public health and the science of firearm injury prevention are in opposition to the US Constitution.
SCIENCE ADVOCACY
Science informs law. Americans’ enjoyment of individual rights and civic security has been repeatedly refined and improved by the application of scientific evidence to legal reasoning. The science of firearm injury prevention intends to diminish firearm-related health risks and, therefore, to improve the rights and securities afforded to all Americans. Portraying firearm injury prevention as being in opposition to Constitutional law expresses a fear of science and the knowledge it may provide. ur profession has long been a standard bearer in injury prevention science. Under the leadership of emergency physicians and other injury prevention specialists, the United States has improved the health outcomes of many nonfatal and fatal injuries, ranging from motor vehicle crashes and drownings to unintentional medication overdoses. These health improvements were achieved without changing the availability of cars, pools, or prescription medications. We have simply made these consumer items, and the behaviors of individuals who use them, safer. We can do the same for firearms, which are by far the most lethal mechanism of injury and which cause the same number of deaths in the United States each year as cars.
FIREARM PREVENTION IN CLINICAL PRACTICE
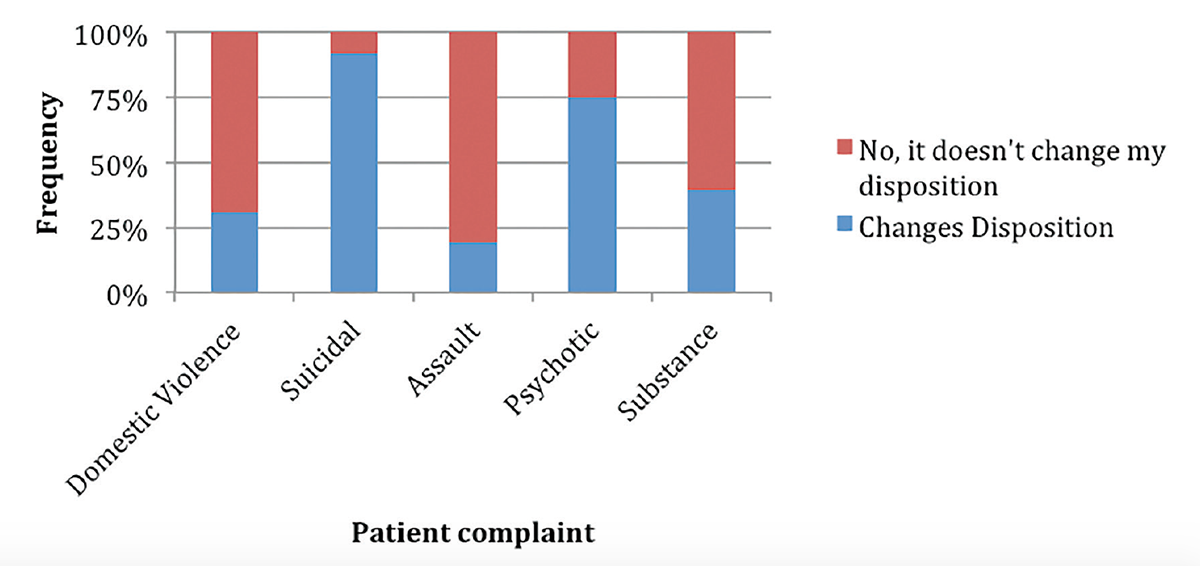
The science of firearm injury prevention also has immediate application to our clinical practice. It’s relevant to every emergency physician who has evaluated the danger of a depressed, angry, agitated, delusional, or intoxicated patient or who has treated a patient at elevated risk of firearm-related victimization or injury/death. According to a recent survey of a sample of emergency physicians participating in the Emergency Medicine Practice Research Network (EM-PRN), the majority of us ask “often” or “almost always” about firearm access for patients with suicidal ideation, with fewer regularly asking about firearm access for patients suffering from psychosis, domestic violence, assault injury, or substance use. More than 90 percent of respondents said that knowledge of firearm access would change their risk assessment and disposition for suicide, and more than two-thirds said that it would change their risk assessment and disposition for victims of domestic violence or patients with acute psychosis (see Figures 1 and 2).

(click for larger image)
Figure 1. Emergency Physician Reported Change in Risk Assessment When Patient Reports Access to Firearm
(click for larger image)
Figure 2. Emergency Physician Reported Change in Disposition When Patient Reports Access to Firearm by Injury Type
Yet most respondents say that their colleagues “almost never” ask suicidal patients about firearm access. Fewer than half of respondents said that they “often” or “almost always” provide lethal means counseling to suicidal patients. The most common reasons that emergency physicians said they didn’t screen were “not having time” and “not knowing what to do with the information” (see Figure 3).

(click for larger image)
Figure 3: Emergency Physician Reported Barriers to Asking About Patient Firearm Access
Of note, only 1 percent of respondents felt that doctors should not ask patients about firearms. This disparity deserves to be addressed. Equally disturbing in this EM-PRN survey, more than half (56 percent) of respondents reported a moderate or high concern about their own safety due to gun violence while working in the emergency department. This safety concern may also be seen through the diffuse deployment and drilling of active-shooter plans in emergency departments, medical offices, and hospitals. As this and other similar data from the peer-reviewed literature show, the risk of firearm injury is an issue of utmost clinical importance to our specialty. As our ability to respond to this problem is clearly underdeveloped, it’s critical for ACEP to continue to advocate for scientific funding to help us mitigate the incidence and health consequences of firearm-related trauma. Emergency physicians need to know how to evaluate for firearm access, whom to screen, and what to do with this information. We need to know how to effectively and quickly mitigate suicide risk among our patients, how best to help victims of domestic violence, and how to reduce the risk of mass violence among our patients with risk factors for violence and access to firearms. Conversations that confuse science and politics distract us from the medically relevant issues of firearm injury risk. This confusion impairs our practice and ultimately harms ourselves, our patients, their families, and our communities.
Dr. Ranney is the past chair of the ACEP Trauma & Injury Prevention Section.
Dr. Barsotti is the chair-elect of the ACEP Trauma & Injury Prevention Section.
Pages: 1 2 3 | Multi-Page




4 Responses to “Opinion: Firearm Injury Prevention Is More Than Pro/Con Debate”
October 22, 2016
Timothy Wheeler, MD“Portraying firearm injury prevention as being in opposition to Constitutional law expresses a fear of science and the knowledge it may provide.”
Fear of science? Really?
The above statement trivializes the truth of the matter, which is abundantly documented–for over two decades organized medicine, starting with the CDC, has waged a very public war on the American civil right of gun ownership. Anyone who seriously contests this is willfully ignoring the historical facts.
Drs. Ranney and Barsotti can read them as easily as anyone else at our website drgo.us .
Timothy Wheeler, MD
Director
Doctors for Responsible Gun Ownership
A Project of the Second Amendment Foundation
October 22, 2016
Dr. Michael S. BrownBy focusing on access to firearms and ignoring access to other mechanisms like flammable liquids and motor vehicles, the authors betray a bias that makes their opinions virtually useless. They are blaming inanimate objects rather than a mental health pathology for bad outcomes. Thinking of this kind is not going to produce better results.
November 6, 2016
Megan RanneyDr. Brown & Dr. Wheeler, thank you for your comments. Dr. Barsotti & I did not ignore access to other mechanisms. We mention in our article that strong and active injury prevention activities have effectively reduced deaths due to other mechanisms.
We urge the use of science to reduce firearm deaths, as well. Firearm injury prevention is NOT the equivalent of being “against guns.” It is being FOR common-sense solutions to reduce firearm injury. These include attention to mental illness; and also include investigating other promising avenues, such as lethal means counseling (for patients who are suicidal) and safety locks (for parents).
We explicitly mention that we don’t know, yet, with certainty, what works. We DO know that airbags, seatbelts, and drunk driving laws work for MVCs – thanks to decades of funding for good science. We need funding for science to figure out what will most effectively reduce firearm injuries and deaths, too. We are glad that you both agree that we need to have thoughtful conversations, and rigorous research, on the topic.
November 27, 2018
Charles Nozicka DO,FAAP,FACEPAmongst modern industrialized nations, only in America do we endure this public health epidemic of firearms related tragedies. On both sides of the gun control debate opinions are lobbed as facts. Neither side listening to the other, unvetted “facts” used as ammunition.
I grew up in a house with guns, learning to shoot before I could drive. I spent many summer days with my grandfather, target shooting with pistols and rifles. He was a life member of the NRA, I am not anti-gun I am anti-gun violence and injury.
It is time to research public safety gun safety best practices and develop strategies for curbing the slaughter within the constraints of the Second Amendment. We all want our families to be safe and live in a country where they do not have to fear some crazed shooter with a self-destructive agenda. We all want to minimize avoidable accidental firearm associated injuries.
The automobile industry collaborating with government has utilized safety research to make our roadways safer. Anti lock brakes, seat belts and crumple technology – save lives everyday. Our cars are registered, tracked with vehicle identification (VIN) numbers. Operators are licensed with mandatory periodic training. Those with health issues are denied driving privileges. The firearm industry must collaborate and partner with us to adopt a similar approach. Congress must foster this partnership – not obstruct it by blocking firearm safety research. We lead the world in firearm related homicide and suicides, if we are going to stop this madness, we must separate our leaders from the NRA and make them accountable to the people who elected them.
Charles Nozicka DO
Division Director
Pediatric Emergency Medicine
Advocate Children’s Hospital
Clinical Professor of Emergency Medicine
Rosalind Franklin University
@RocketDoc53