Explore This Issue
ACEP Now: Vol 33 – No 11 – November 2014(click for larger image)
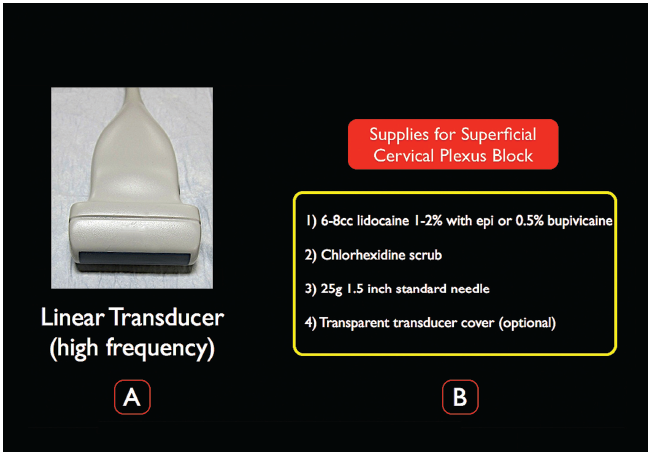
Figure 2.
A) A high-frequency linear transducer is ideal for the ultrasound-guided SCP block. B) Supplies needed for the SCP block.
Survey Scan. Place the patient in lateral decubitus position, with the affected side facing up. The ultrasound system should be located contralateral to the affected side, allowing the clinician to comfortably view the screen and the site of injection. Place a high-frequency linear transducer (15-6 MHz) in a transverse plane on the anterior neck at the level of the thyroid cartilage (probe marker pointing medially toward the thyroid). Clinicians who perform ultrasound-guided CVC should be familiar with the sonoanatomy at this level and be able to visualize the internal jugular vein, carotid artery, thyroid, and sternocleidomastoid muscle (Figure 3A). From this familiar position, the probe should be moved cephalad to the C4 level (the superior pole of the thyroid cartilage) and then laterally until the SCM muscle tapers to a beak (Figure 3B). The SCP is located just under the SCM and will be noted as a hyperechoic structure below the SCM and just above the levator scapulae muscle (LSM). Visualization of the interscalene groove or components of the brachial plexus indicates a low position; at the target C4 level, scalene muscles are typically quite small, deep, or not visualized (Figure 3B).
(click for larger image)
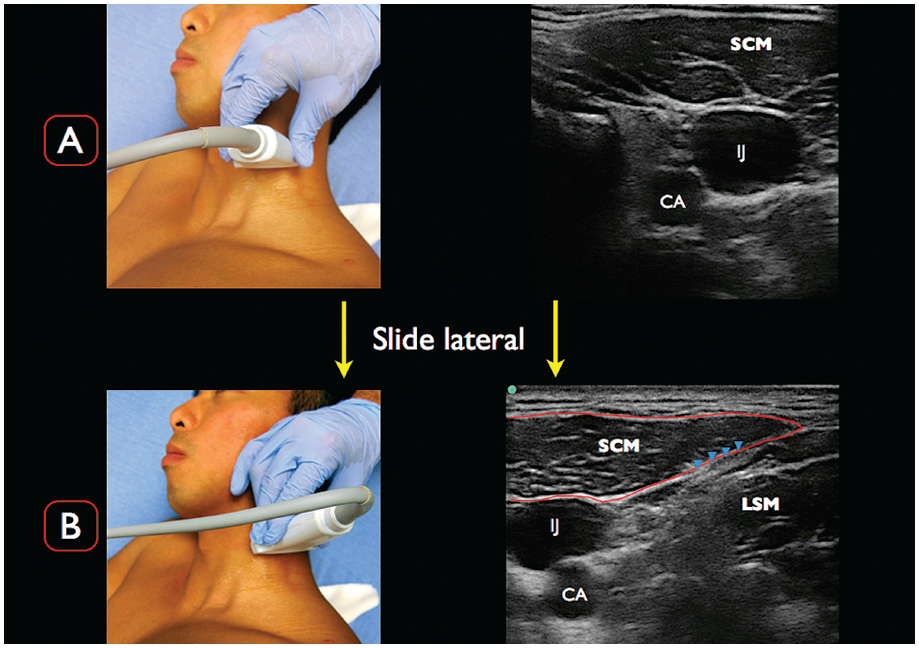
Figure 3.
A) Place the transducer in a transverse orientation to the neck at the superior portion of the thyroid cartilage. Note the classic ultrasonographic landmarks; CA= carotid artery; IJ= internal jugular vein; SCM= sternocleidomastoid muscle. B) At the level of the superior portion of the thyroid cartilage, slowly slide the transducer laterally. Note the tapering of the SCM muscle and the LSM just below. The superior cervical plexus (SCP denoted by the blue arrowheads) is the group of hyperechoic structures between the SCM muscle and LSM.
Other commonly used landmarks to ensure the correct cervical level of the SCP block include the midpoint of the SCM from the mastoid to its insertion on the clavicle and the point where the external jugular crosses the posterolateral border of the SCM.
Needle Insertion and Injection. The patient should be placed on continuous cardiac monitoring. Attach a 10 cc syringe filled with 6–8 cc of local anesthetic (eg, bupivacaine 0.5% or lidocaine 1%) to a 25 g 1.5″ needle. After the transducer is placed in a transverse position over the anterior neck, we recommend using color Doppler to confirm the lack of aberrant vasculature. An in-plane posterior approach (lateral to medial) will allow the clinician to clearly visualize the needle during the entire nerve block. The goal is to guide the needle tip just under the tapering posterolateral edge of the SCM to the fascial layer between the SCM and LSM (Figure 4). Gentle aliquots of anesthetic should be placed in this location, ensuring anechoic spread of fluid on the ultrasound screen. Common errors include nonvisualized anesthetic spread and/or placing the needle tip in either the SCM or levator scapulae muscle belly.
Pages: 1 2 3 | Single Page




One Response to “Pain Control Using Ultrasound-Guided Superficial Cervical Plexus Block”
October 19, 2021
Hazel McArdleCan ultrasound be used for scalene tight muscles