Explore This Issue
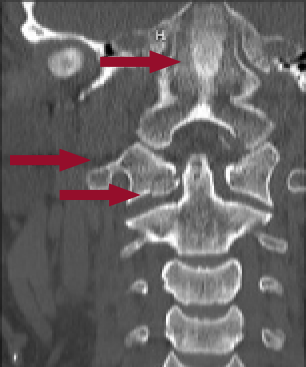
ACEP Now: Vol 41 – No 01 – January 2022Figure 1: CT showing a C1 fracture with evidence of retroclival hemorrhage extending through foramen magnum. Facets at C1–C2 are no longer aligned.
Atlanto-occipital dissociation (AOD) is often the result of high-velocity trauma injuries.1 It is believed that AOD may have a higher incidence than previously estimated due to the number of cervical spine (C-spine) injuries that resulted in death with AOD having been found on postmortem examinations.
The Case
A 30-year-old woman initially presented to a small community emergency department following a motor vehicle crash. The patient was a restrained driver in a sedan that was T-boned by a pickup truck in an intersection at high speed. The patient had a prolonged extraction, with initial Glasgow Coma Score (GCS) of 5. EMS was unable to intubate with direct laryngoscopy in the field but was able to use a bag valve mask effectively until arrival at the emergency department. C-spine precautions were maintained throughout the prehospital and hospital settings.
During the prompt primary survey, the patient was intubated due to having a GCS of 3. The patient subsequently had a one-view chest X-ray to confirm placement and was quickly transferred to the Level 1 trauma center. Upon arrival to our emergency department, the patient was assessed by an emergency medicine resident, the emergency medicine attending, and the trauma team. The patient was arousable, with a GCS of 10T. She was moving all extremities and demonstrated minimal external signs of trauma; however, she may have had mildly decreased sensation on the right side. The patient was quickly sent to CT following the primary survey, focused assessment with sonography in trauma (FAST), X-rays, and secondary survey. Despite the patient’s well appearance, her C-collar remained on and C-spine precautions were kept.
Following CT, we received an urgent call from the radiologist that the CT demonstrated a retroclival hemorrhage extending through the foramen magnum with mass effect on the medulla and upper cervical spinal cord, as well as a displaced type 3 left occipital condylar fracture and mildly displaced fracture through right anterior C1 arch (See Figure 1). The neurosurgery consult note read, “Atlanto-occipital dissociation injury—extremely unstable, skull is detached from C-spine. Typically, this injury is immediately fatal in about 80% of cases.”
Discussion

Figure 2: MRI showing a subdural hematoma at the cervical medullary junction causing stenosis to the spinal canal just inferior to the foramen magnum
Jordan Stav
Despite AOD having extremely high mortality and morbidity, there have been increasing reports of AOD survivors.1 The decrease in morbidity and mortality may be due to the advents of prehospital care as well as the early recognition and treatment in the emergency department, which has been associated with the establishment and development of emergency medicine as a specialty.1–3
The earlier the patient is put in C-spine stabilization and advanced imaging is performed—often with CT, then MRI—the greater the probability of improved morbidity and mortality.4 Following external stabilization and diagnosis, early and aggressive surgical stabilization is associated with improved outcomes.5
Due to the decrease in mortality, AOD may become a more frequent diagnosis in the emergency department. It is important that we keep C-spine injuries at the forefront of our minds while evaluating trauma patients. This entails maintaining C-spine precautions during procedures and transport of these patients.
Case Resolution
This patient was taken to the operating room for emergent neurosurgical intervention following her MRI findings (See Figure 2). Her occiput was fused to C2. The patient was subsequently successfully extubated and discharged home six days after her surgery. She was able to walk out of the hospital under her own strength and has had an uneventful recovery to date.
 Dr. Stav is a PGY3 emergency medicine resident at Ascension Macomb-Oakland Hospital in Warren, Michigan. DR. KOPP, DR. MA, and DR. DAOUK are emergency physicians at Ascension St. John Hospital in Detroit.
Dr. Stav is a PGY3 emergency medicine resident at Ascension Macomb-Oakland Hospital in Warren, Michigan. DR. KOPP, DR. MA, and DR. DAOUK are emergency physicians at Ascension St. John Hospital in Detroit.
References
- Ehlinger M, Charles YP, Adam P, et al. Survivor of a traumatic atlanto-occipital dislocation. Orthop Traumatol Surg Res. 2011;97(3):335-340.
- Hall GC, Kinsman MJ, Nazar RG, et al. Atlanto-occipital dislocation. World J Orthop. 2015;6(2):236-243.
- Garrett M, Consiglieri G, Kakarla UK, et al. Occipitoatlantal dislocation. Neurosurgery. 2010;66(3 Suppl):48-55.
- Saeheng S, Phuenpathom N. Traumatic occipitoatlantal dislocation. Surg Neurol. 2001;55(1):35-40; discussion 40.
- Hadley MN, Walters BC, Grabb PA, et al. Diagnosis and management of traumatic atlanto-occipital dislocation injuries. Neurosurgery. 2002;50(3 Suppl):S105-113.
Pages: 1 2 3 | Multi-Page


No Responses to “Serious C-Spine Injuries Are Becoming More Common—and Survivable”