Chronic knee pain is common and debilitating. Patients often seek care in the emergency department (ED) setting when flares of pain affect their ability to ambulate, climb stairs, or even stand up from sitting.1 In many cases, these patients have been dealing with pain for years and have already exhausted the standard analgesic cocktail of acetaminophen, NSAIDs, and/or topical agents. Patients and clinicians are both aware of the obvious downstream risks of adding opioids to this multimodal regimen. Intra-articular steroid injections can be an excellent option but come with their own risks given they violate the joint space and are not commonly performed in the ED setting. The genicular nerve block offers a simplified, safe alternative for treating severe knee pain. In conjunction with multimodal oral and topical pain regimens, this motor sparing block can provide both acute pain control and lasting relief for weeks to months following the injection for patients with severe knee pain.2,3
Explore This Issue
ACEP Now: Vol 43 – No 05 – May 2024Sonoanatomy
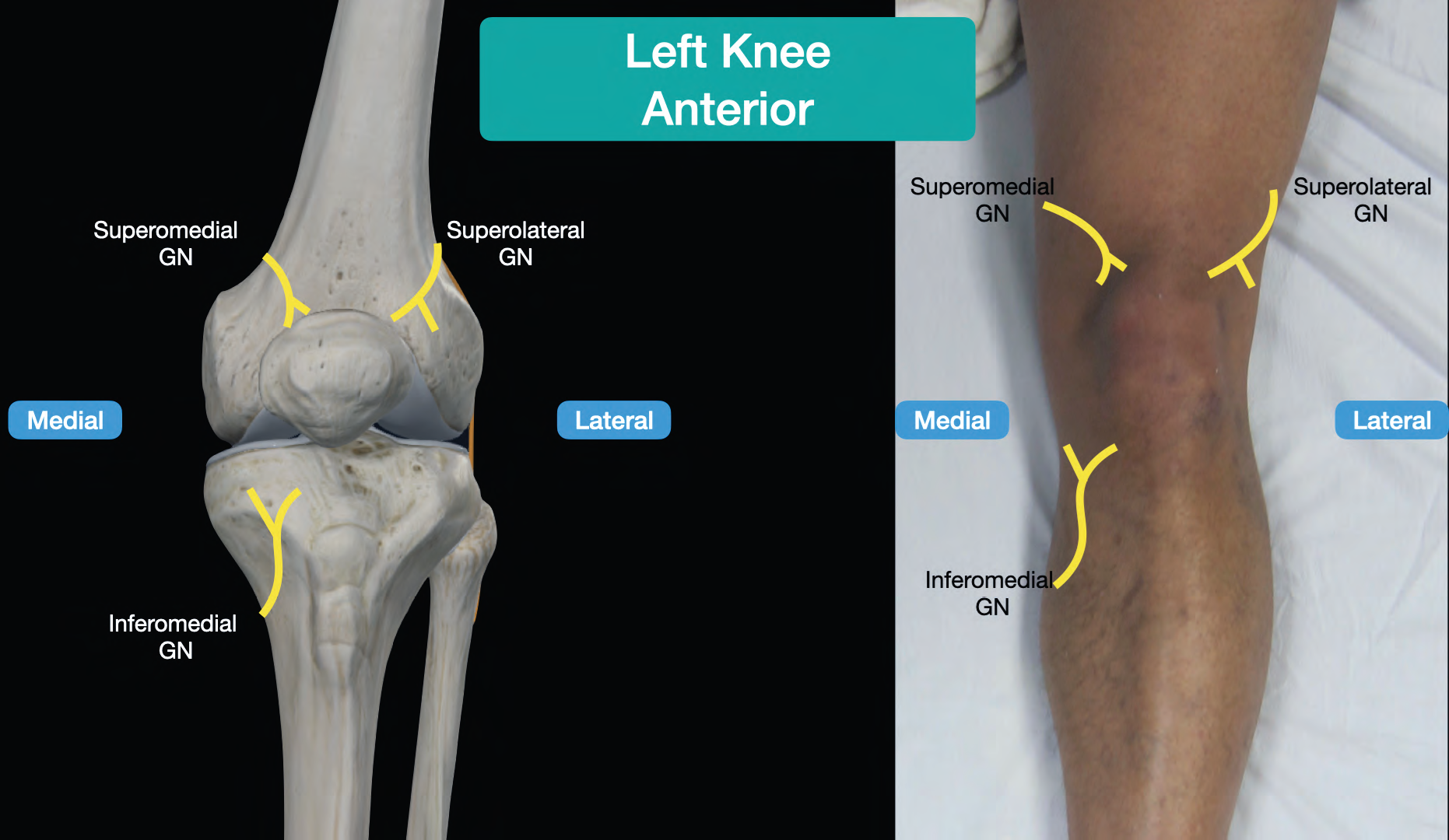
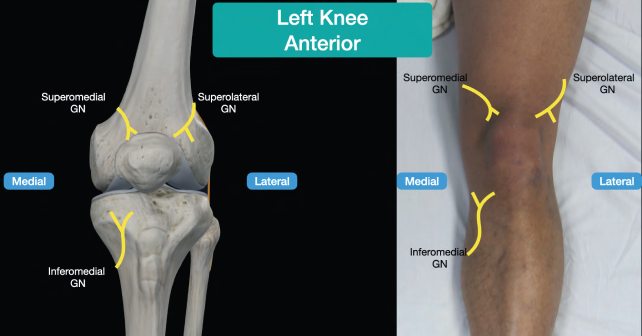
FIGURE 1. Bony and surface anatomy of the knee with the superomedial, superolateral, and inferomedial nerves shown. Note that the inferolateral genicular nerve is omitted as this is not blocked to avoid foot drop from the nearby superficial peroneal nerve. (Click to enlarge.)
The innervation of the knee is complex, but much of its sensory innervation is supplied by the genicular nerves, which are easy targets for ultrasound-guided nerve blocks. The genicular nerves are a group of four sensoryonly branches (off of the sciatic nerve) that wrap around the femoral condyles superiorly and the proximal tibia and fibula inferiorly. The genicular nerves are named based on their corresponding quadrant of the knee joint (superolateral, superomedial, inferomedial, and inferolateral) and run immediately adjacent to the bone, following the course of the genicular arteries. Their proximity to the bone allows us to use the bone as a backstop for the needle, making this a particularly easy block to perform. The genicular nerve block targets the superolateral, superomedial and inferomedial genicular nerves. We recommend not blocking the inferolateral nerve because of its close proximity to the superficial peroneal nerve and possibility of inadvertently causing a foot drop.
How to Perform the Block
Supplies
- High frequency linear transducer
- Chlorhexidine
- Block needle
- Probe cover
- Sterile gel
- 3 mL lidocaine 1 percent for skin with 25g needle
- 10 mL bupivacaine 0.5 percent mixed with 10 mg dexamethasone
Step 1
Prepare a 5 mL syringe with 3-5 mL of lidocaine 1 percent for skin wheals at each site of needle entry. Prepare another syringe with 10 mL of bupivacaine 0.5 percent and 10 mg dexamethasone. Place the patient supine with the knee exposed. Disinfect the anterior aspect of the knee with chlorhexidine and place a transparent adhesive cover on the probe.
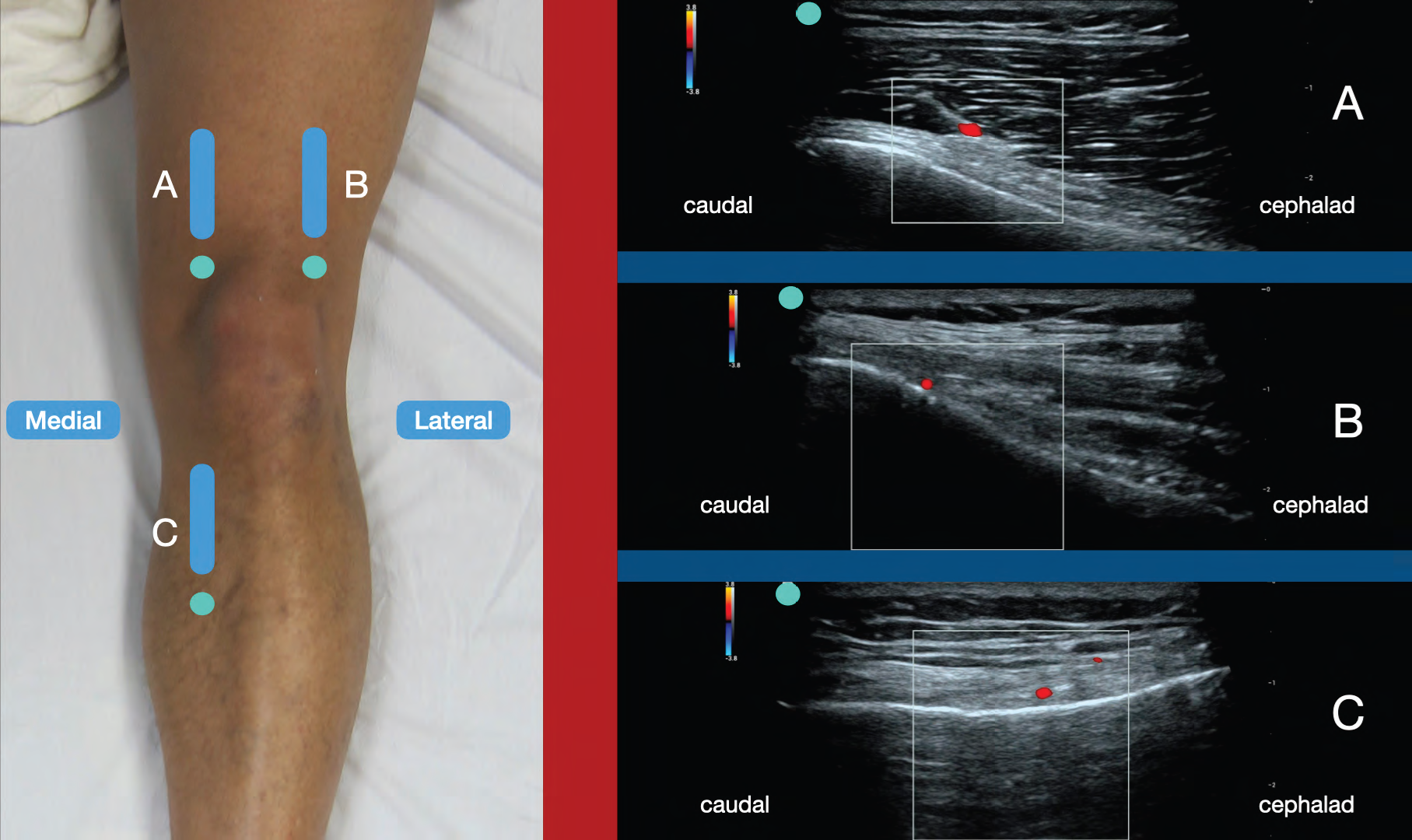
FIGURE 2. Probe placement (probe marker in green) and corresponding ultrasound images for the superomedial (A), superolateral (B), and inferomedial (C) genicular nerves with color Doppler showing the corresponding genicular arteries. (Click to enlarge.)
Step 2
Place the ultrasound system contralateral to the affected knee so that you have a clear line of sight of the ultrasound screen when performing the block. The three locations for anesthetic deposition are the superomedial, superolateral, and inferomedial genicular nerves. The goal of this block is to gently place the needle tip against the bone at each location and spread local anesthetic along the surface of the periosteum toward the nerve.
Step 3
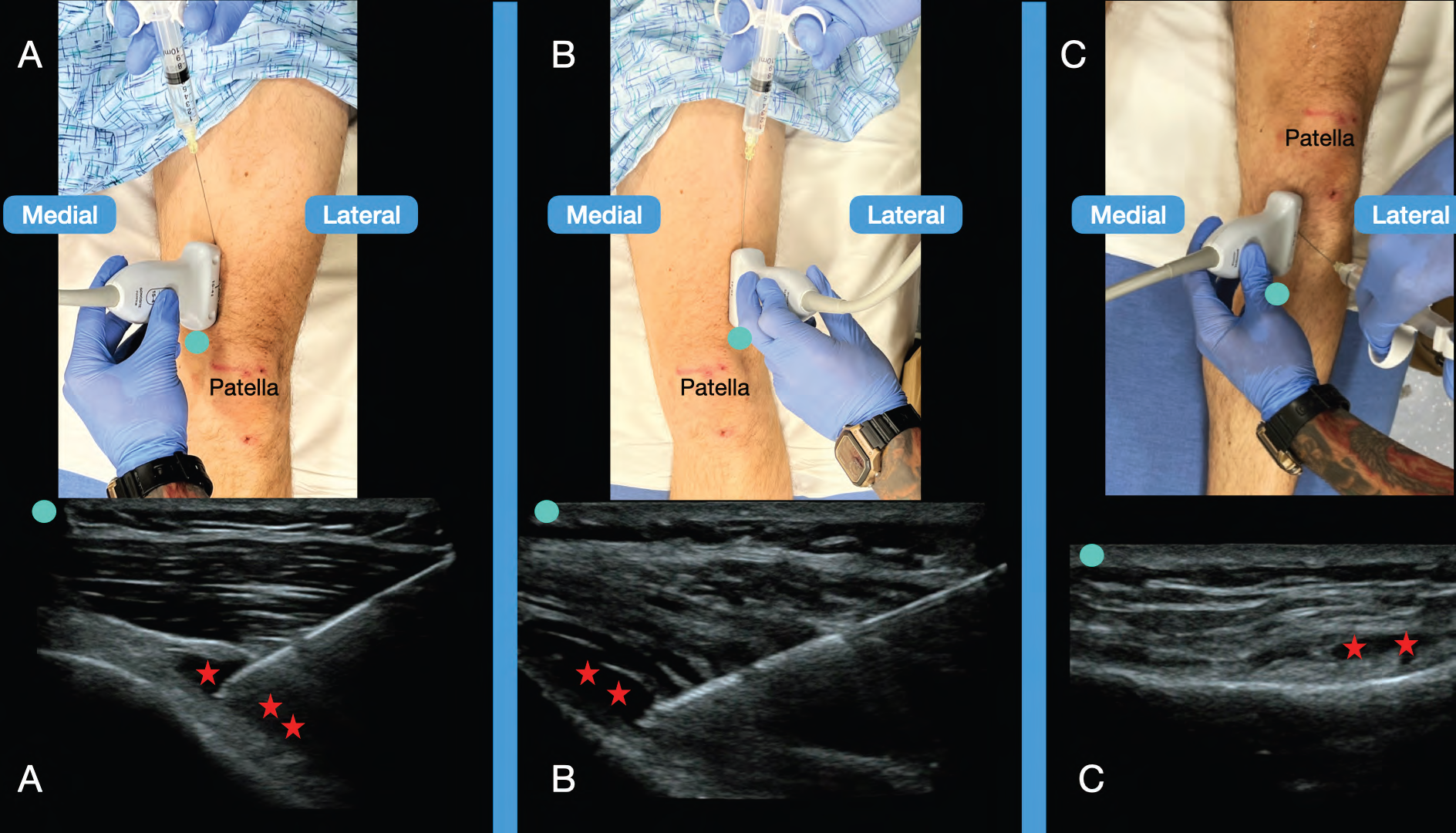
FIGURE 3. Probe and needle placement with corresponding ultrasound images demonstrating needle positioning and post-injection local anesthetic spread between the muscle and bone (red star) at the superomedial (A), superolateral (B), and inferomedial (C) sites. (Click to enlarge.)
For the superomedial and superolateral genicular nerves, the probe is placed longitudinally just proximal to the knee joint to identify where the femoral shaft curves outward toward the condyles. The medial and lateral sides should appear nearly identical. Identification of the genicular arteries with color Doppler can be attempted but can be difficult because of their small size. Anesthetize the skin with 1 mL of 1 percent lidocaine, then advance the block needle down to the bone. Aspirate prior to injecting to prevent inadvertent intravascular injection and inject 3-4 mL of long-acting anesthetic mixed with corticosteroid at each site. Ensure that anechoic fluid spreads along the femur. We prefer an in-plane, superior to inferior approach, but an out-of-plane technique can be performed, as well.4
The inferomedial genicular nerve is about 3 cm medial to the tibial tuberosity (similar to the site used for intra-osseous access), where the surface of the tibia forms a shallow bowl. The probe is placed longitudinally and color Doppler can be used to identify the genicular artery. Anesthetize the skin and insert the block needle, using an out-of-plane approach, down to bone, taking care to avoid the artery. An out-of-plane technique is used for this portion of the block because of the shallow depth of the target. After negative aspiration, inject 3-4 mL of long-acting anesthetic mixed with corticosteroid along the bone.
This adapted technique from our anesthesia colleagues does not provide complete surgical anesthesia, but rather significant sensory analgesia. In our experience, patients have been able to ambulate comfortably with no motor deficits in approximately 30 minutes. Also, the very low volumes needed for this block allows for the possibility of performing bilateral blocks with safe anesthetic volumes.
Conclusion
The ultrasound-guided genicular nerve block is a safe, simple technique for treating acute on chronic knee pain. The block provides both the immediate relief that the patient desires and sustained functional improvement that will help prevent bouncebacks, while avoiding the risks associated with opioid prescriptions or injections that violate the joint space. This block is commonly offered in outpatient pain clinics but can be easily adapted to the ED setting.5,6
Dr. Stegeman is an Ultrasound Fellow at Alameda Health System / Highland Hospital.
Dr. Mikell is an Ultrasound Fellow at Alameda Health System / Highland Hospital.
Dr. Martin is the Ultrasound Fellowship Director at Alameda Health System / Highland Hospital.
Dr. Nagdev is the Ultrasound Division Director, Alameda Health System / Highland Hospital.
References
- Gwam CU, Etcheson JI, George NE, Mistry JB, Mohamed N, Patel A, Gwam PN, Piuzzi NS, Delanois RE. Presentation of Knee Osteoarthritis in the Emergency Department: A Problem Worth Mentioning? Surg Technol Int. 2017 Dec 22;31:277-284.
- Ragab, A.R., Hegab, S., Elnemr, R. et al. Intra-articular corticosteroid injection and genicular nerve block under ultrasound guidance in pain control of knee osteoarthritis. Egypt J Radiol Nucl Med. 52, 196 (2021).
- Kim DH, Choi SS, Yoon SH, Lee SH, Seo DK, Lee IG, Choi WJ, Shin JW. Ultrasound-Guided Genicular Nerve Block for Knee Osteoarthritis: A Double-Blind, Randomized Controlled Trial of Local Anesthetic Alone or in Combination with Corticosteroid. Pain Physician. 2018 Jan;21(1):41-52.
- Dunworth S, Gadsden J. How I do it: genicular nerve blocks for acute pain. ASRA Pain Medicine News. 2022;47.
- Sobel J, Oswald J. Novel Use of 3-Point Genicular Nerve Block for Acute Knee Pain in the Emergency Department. J Emerg Med. 2021 Oct;61(4):416-419. Epub 2021 Jun 25.
- Kong C, Bubic IJ, Tran AA, Tan G, Medak AJ, Oswald J. Genicular nerve block for emergency department patient: a successful management of subacute osteoarthritic knee pain. Pain Manag. 2023 Jul;13(7):373-378. Epub 2023 Jul 17.
Pages: 1 2 3 | Multi-Page




No Responses to “The Ultrasound-Guided Genicular Nerve Block”