
Case
A 50-year-old woman presents to the emergency department (ED) complaining of epigastric pain and nausea for 36 hours. The physical examination is consistent with biliary colic and the blood work shows a mild elevation in C-reactive protein while her white blood cell count and liver function tests are normal. You perform a biliary ultrasound (US) in the ED (BUSED) which shows a gallbladder (GB) full of stones, some GB wall thickening and a positive Murphy’s sign. Will this be enough for the general surgeon, or will they want an US performed by the radiology department to make their surgical decision?
Explore This Issue
ACEP Now: Vol 42 – No 07 – July 2023Clinical Question
What is the value of radiology-performed US (RUS) compared to BUSED in terms of the surgical decision-making in acute biliary disease?
Click to enlarge.
Background
Ultrasound is typically the first-line imaging modality for the diagnosis of acute biliary disease. ED physician-performed point of care ultrasound (POCUS) has increased in popularity over the last decade. Several small trials have compared the accuracy of POCUS versus the “gold standard” of radiology performed ultrasound. Little is known regarding whether the department in which the US is performed (ED or radiology) impacts the surgeon’s clinical decision making.
Reference: Hilsden, et al. Point of care biliary ultrasound in the emergency department (BUSED) predicts final surgical management decisions. Trauma Surg Acute Care Open. 2022;7(1):e000944.
- Population: Adult ED patients 18 years of age or older with abdominal pain whom the EM physician felt had biliary disease after performing a history, physical examination, and BUSED.
- Excluded: Cases in which surgery was completed prior to formal ultrasound imaging, there was failure to gain consent, or patient’s age was less than 18 years.
- Intervention: Surgical decision (offer surgery, endoscopic retrograde cholangiopancreatography/magnetic resonance cholangiopancreatography [ERCP/MRCP], or no surgery) based on the clinical, laboratory and BUSED data. There were 11 specially trained ED physicians and 20 surgeons.
- Comparison: Surgical decision made after formal radiology ultrasound (RUS).
- Outcome (Primary): Percentage of patients in which the management changed after RUS was performed.
- Type of Study: Observational, prospective, cohort study performed at a tertiary care center in Canada.
Authors’ Conclusions

Gallstones removed via surgery.
This prospective study has shown that in the vast majority of cases the additional information afforded by formal RUS does not alter clinical management. Point-of-care biliary ultrasound has been demonstrated to be reliable in the diagnosis of acute biliary disease and offers a safe and efficient diagnostic pathway for patients presenting in the emergency department.
Results
There were 100 consecutive patients recruited into the study available for analysis. The mean age of participants was 50 years. They admitted 68 patients for surgery, 21 for duct clearance (ERCP/MRCP), and 11 for no surgery.
Key Result
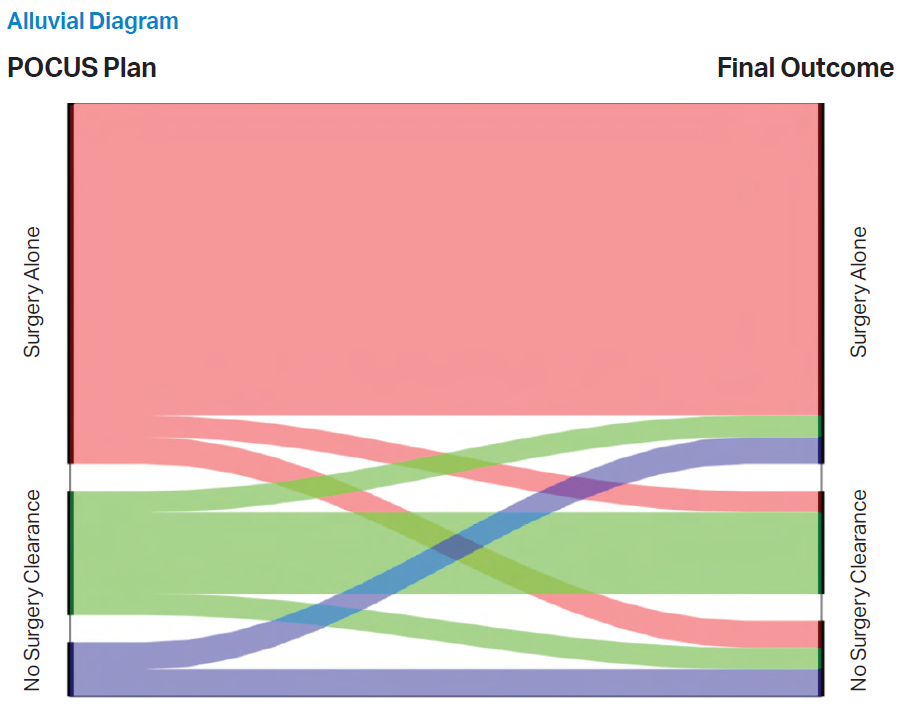
- The surgical plan was not changed often after a formal radiology US was performed.
- Primary outcome: The initial plan based upon the ED POCUS was changed 10 percent of the time after RUS was performed. See the alluvial diagram.
EBM Commentary
- Unmasked surgeons: The surgeon in this study knew that the patient was going to have both a BUSED and RUS examination. This could have introduced some confounders depending on the surgeon’s opinion of BUSED. This issue could have been addressed by masking the surgeon to which report was from the ED and which was a formal US from the radiology department.
- External validity: This is a small study of 11 emergency physicians and 20 surgeons performed at a single, tertiary, university-affiliated hospital in Canada. Hospitals have their own culture of practice patterns. This group of physicians may not reflect practice in other tertiary centers, smaller community hospitals, or different countries.
- Location versus experience: Ultimately, this is not a comparison between BUSED and RUS, but between US and US. The skill to obtain and interpret an US image is operator-dependent. It can be tricky to detect gallstones in the neck of the GB or common bile duct; it is a learned skill. Sensitivity for these subtle findings goes up with experience. The difference observed in this study could be due to less-experienced versus more-experienced sonographers.
Bottom Line
An emergency physician trained in BUSED can correctly inform surgical decision-making in most cases of non-jaundiced adult patients with suspected acute biliary disease.
Case Resolution
You present the surgeon with the clinical case, including the BUSED results. The surgeon agrees the patient has acute cholecystitis and admits the patient to the surgical team for further management.
Remember to be skeptical of anything you learn, even if you heard it on the Skeptics’ Guide to Emergency Medicine.
Thank you to Dr. Casey Parker, an emergency physician working in Broome, Australia, for his help with this review.
Pages: 1 2 | Multi-Page




No Responses to “Using Ultrasound to Make Surgical Decisions in Suspected Biliary Colic”